You might also like
- Pediatric Case Presentation 1Document4 pagesPediatric Case Presentation 1soso122100% (1)
- IVMS Hematology-Oncology Summary Table-Notes For USMLE Step 1 Prep.Document16 pagesIVMS Hematology-Oncology Summary Table-Notes For USMLE Step 1 Prep.Marc Imhotep Cray, M.D.100% (1)
- CH50Document88 pagesCH50ABIGAILNo ratings yet
- Complement SystemDocument62 pagesComplement SystemYelai CarveroNo ratings yet
- Transfusion MedicineDocument274 pagesTransfusion MedicineZuhair BarazanchiNo ratings yet
- Antibodies: Type Response Action Other Hypersensitivity TypeDocument2 pagesAntibodies: Type Response Action Other Hypersensitivity TypemcwnotesNo ratings yet
- Complement: Dr. Mohamed El-Azizi Dr. Mohamed El-AziziDocument51 pagesComplement: Dr. Mohamed El-Azizi Dr. Mohamed El-AziziMirette AshrafNo ratings yet
- Imse Midterm Reviewer - Pacate, Joyce C.Document21 pagesImse Midterm Reviewer - Pacate, Joyce C.jcpacate1178qcNo ratings yet
- Adaptive Immunity: Mateen IrfanshaDocument42 pagesAdaptive Immunity: Mateen IrfanshaNabil holmesNo ratings yet
- Complementsystem UpdatedDocument41 pagesComplementsystem UpdatedMadhumita PandaNo ratings yet
- Lesson 6 ComplementDocument8 pagesLesson 6 ComplementYzza DerequitoNo ratings yet
- Immunology:: Unit 7-The Complement SystemDocument6 pagesImmunology:: Unit 7-The Complement SystemCyreen Jill AlilingNo ratings yet
- Class 2inflammationDocument70 pagesClass 2inflammationAfifa AfrozNo ratings yet
- Basic Immunology: Presented By-Dr. Prachi MulayDocument42 pagesBasic Immunology: Presented By-Dr. Prachi MulayPrachi MulayNo ratings yet
- The Biological Functions of The Complement SystemDocument9 pagesThe Biological Functions of The Complement SystemAishah NajihahNo ratings yet
- Complement SystemDocument30 pagesComplement SystemxNo ratings yet
- The Complement System: - Neeraja. ADocument23 pagesThe Complement System: - Neeraja. AGayathri deviNo ratings yet
- B CELLS SeminarDocument81 pagesB CELLS SeminarviolaNo ratings yet
- Complement SystemDocument28 pagesComplement SystemRONAK LASHKARINo ratings yet
- The Complement System: By: Dr. Suzan YousifDocument36 pagesThe Complement System: By: Dr. Suzan YousifSai BabaNo ratings yet
- Complement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtDocument70 pagesComplement: Kathleen Basa Kris Nicole de Guzman Jessica Mae Ong 3HmtCherry Reyes-Principe100% (1)
- Complement SystemDocument6 pagesComplement SystemApril Love RetizaNo ratings yet
- The Complement SystemDocument38 pagesThe Complement SystemIraqiNo ratings yet
- Immunology PharmagupshupDocument10 pagesImmunology PharmagupshupSHRIKANTNo ratings yet
- Immunology Course SummaryDocument30 pagesImmunology Course SummaryKiller VNo ratings yet
- Dr. Pratiwi S Gunawan, Drg.,Mkes.,Pah (K)Document31 pagesDr. Pratiwi S Gunawan, Drg.,Mkes.,Pah (K)Bima Ewando KabanNo ratings yet
- 1 - Cells of Immunity - Complement - FontDocument75 pages1 - Cells of Immunity - Complement - FontMoneeshNo ratings yet
- Celulas T y SeñalizacionDocument129 pagesCelulas T y SeñalizacionAnghela CalderónNo ratings yet
- Complement System TherapeuticsDocument36 pagesComplement System Therapeuticsmurfiqahharizah03No ratings yet
- Complement SystemDocument4 pagesComplement SystemFait HeeNo ratings yet
- Complement System, Its Activation Pathways, Functions in The Formation of Immune Response To An Antigen.Document25 pagesComplement System, Its Activation Pathways, Functions in The Formation of Immune Response To An Antigen.Helena Pascual PérezNo ratings yet
- Lect. 4 The Complement Proteins and Their ReceptorsDocument15 pagesLect. 4 The Complement Proteins and Their ReceptorsMuhammadNo ratings yet
- IMMUNOLOGYDocument21 pagesIMMUNOLOGYNicole AguilarNo ratings yet
- Sesi 1 - DR - Umi - Imunologi Transfusi DarahDocument46 pagesSesi 1 - DR - Umi - Imunologi Transfusi DarahWanda RyNo ratings yet
- Adaptive Immunity - 1Document15 pagesAdaptive Immunity - 1FN FajrinNo ratings yet
- Carroll 2004Document7 pagesCarroll 2004Luan dos PNo ratings yet
- ImmunologyDocument32 pagesImmunologympume lisahNo ratings yet
- The Complement SystemDocument4 pagesThe Complement SystemExamville.com100% (1)
- KA P:S - The Lazy OCD VersionDocument9 pagesKA P:S - The Lazy OCD VersionsaialamNo ratings yet
- Antigen Recognition in The Adaptive Immune System: Agussalim BukhariDocument21 pagesAntigen Recognition in The Adaptive Immune System: Agussalim BukhariinhaNo ratings yet
- L1c Complement SystemDocument39 pagesL1c Complement Systemashutoshrath209No ratings yet
- DR A.Aziz Djamal MSC - DTM&H.SPMK (K)Document27 pagesDR A.Aziz Djamal MSC - DTM&H.SPMK (K)Irfan GhaniNo ratings yet
- Complement System-1Document22 pagesComplement System-1Way INo ratings yet
- Overview of Complement Activation and RegulationDocument14 pagesOverview of Complement Activation and RegulationAnna SkrobińskaNo ratings yet
- Janeway Chapter Question AnswersDocument9 pagesJaneway Chapter Question AnswersNguyễn Nam AnhNo ratings yet
- APC-C ComplexDocument13 pagesAPC-C ComplexJoshua OriokoNo ratings yet
- T4 Complement SystemDocument42 pagesT4 Complement Systemกฤติน วนิจวรางกุลNo ratings yet
- Complement (Yt)Document7 pagesComplement (Yt)Vince Martin ManaigNo ratings yet
- Ancient InteractionsDocument11 pagesAncient InteractionsNuria Areli Márquez PérezNo ratings yet
- Immunity SummaryDocument4 pagesImmunity SummaryVishnuga MohanNo ratings yet
- Seminar Presentation: Title: The Complement SystemDocument7 pagesSeminar Presentation: Title: The Complement SystemafricanusquintusNo ratings yet
- Komplemen: Bambang Heru BudiantoDocument38 pagesKomplemen: Bambang Heru Budiantoliana_ameyliaNo ratings yet
- 2 The Complement SystemDocument40 pages2 The Complement SystemJohn Louis RanetNo ratings yet
- The International Journal of Biochemistry & Cell Biology: Complement Component 5a (C5a)Document4 pagesThe International Journal of Biochemistry & Cell Biology: Complement Component 5a (C5a)FrontiersNo ratings yet
- CompletementDocument3 pagesCompletementzeythu1No ratings yet
- Complement SystemDocument6 pagesComplement SystemJimit GandhiNo ratings yet
- Complement 2015 PDFDocument31 pagesComplement 2015 PDFSetiawan DonnieNo ratings yet
- AntibodyDocument47 pagesAntibodyChelly JimenoNo ratings yet
- Immunology: Key FeaturesDocument18 pagesImmunology: Key FeaturesmusatiiNo ratings yet
- Function, Structure and Therapeutic Potential of Complement C5a ReceptorsDocument20 pagesFunction, Structure and Therapeutic Potential of Complement C5a ReceptorsFrontiersNo ratings yet
- CBC Pratice OHS ProceduresDocument6 pagesCBC Pratice OHS ProceduresRonelene GatoNo ratings yet
- List of Consumables - RohDocument2 pagesList of Consumables - RohRonelene GatoNo ratings yet
- Course DesignDocument64 pagesCourse DesignRonelene GatoNo ratings yet
- Competency Based Curriculum - Concoctions and ExtractsDocument5 pagesCompetency Based Curriculum - Concoctions and ExtractsRonelene GatoNo ratings yet
- F11 - Competency Based Curriculum - VEGDocument6 pagesF11 - Competency Based Curriculum - VEGRonelene GatoNo ratings yet
- FARM PLANNING AND DECISION - MAKING Final2Document16 pagesFARM PLANNING AND DECISION - MAKING Final2Ronelene GatoNo ratings yet
- Orientation For The TraineesDocument19 pagesOrientation For The TraineesRonelene GatoNo ratings yet
- Biroi HiveDocument6 pagesBiroi HiveRonelene GatoNo ratings yet
- Biroi HiveDocument6 pagesBiroi HiveRonelene GatoNo ratings yet
- BDH Mti Phleb Notes 2022Document114 pagesBDH Mti Phleb Notes 2022Ronelene GatoNo ratings yet
- MUST To KNOW in HematologyDocument46 pagesMUST To KNOW in HematologyRona Salando100% (2)
- Interpret HbA2 With Caution Per DR Barbara BainDocument50 pagesInterpret HbA2 With Caution Per DR Barbara Baindamadol100% (1)
- J.Jass, S.Surman, J.Walker - Medical Biofilms - Detection, Prevention and Control, 2003 PDFDocument305 pagesJ.Jass, S.Surman, J.Walker - Medical Biofilms - Detection, Prevention and Control, 2003 PDFSorinaLuciaNo ratings yet
- Guillian-Barre Syndrome: Renalyn Galache Gladys Gegare BSN-3BDocument18 pagesGuillian-Barre Syndrome: Renalyn Galache Gladys Gegare BSN-3BGLadys GegareNo ratings yet
- Biology ProjectDocument52 pagesBiology ProjectBhagat Bhandari67% (3)
- Parasitology-Lec 7 Lung FlukesDocument5 pagesParasitology-Lec 7 Lung Flukesapi-3743217100% (1)
- Introduction To AntibioticsDocument9 pagesIntroduction To AntibioticsRishabh Narula100% (1)
- What Causes Food Spoilage?: Melissa H. Pecundo IAS-BiologyDocument12 pagesWhat Causes Food Spoilage?: Melissa H. Pecundo IAS-BiologyAbie Jewel Joy RoqueNo ratings yet
- Spread of Canine Influenza A (H3N2) Virus, United StatesDocument8 pagesSpread of Canine Influenza A (H3N2) Virus, United StatesAde GunawanNo ratings yet
- 00 Communicable DiseasesDocument8 pages00 Communicable DiseasesAngelica AlayonNo ratings yet
- Waj 3101Document4 pagesWaj 3101Siti Nur AmalinaNo ratings yet
- Korea Ghsa 2019Document283 pagesKorea Ghsa 2019BRAAAP SQRTNo ratings yet
- RUHS Pre PG 2014 MBBS Section II Question Paper and Answer KeyDocument18 pagesRUHS Pre PG 2014 MBBS Section II Question Paper and Answer KeyAnweshaBoseNo ratings yet
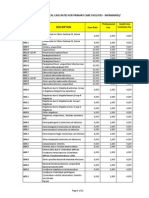
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraNo ratings yet
- Intrapartum CareDocument65 pagesIntrapartum Caremarkus_danusantosoNo ratings yet
- Topic 1 PseudomonashhjjunDocument8 pagesTopic 1 PseudomonashhjjunRachel Marie M. GaniaNo ratings yet
- (MICRO2) Gram Negative CocciDocument41 pages(MICRO2) Gram Negative CocciMadhu MithaNo ratings yet
- UNIT TEST-Pathogens and DiseaseDocument15 pagesUNIT TEST-Pathogens and DiseaseElizabeth McallisterNo ratings yet
- Controlling Microbial Growth in Vivo Using Antimicrobial AgentsDocument30 pagesControlling Microbial Growth in Vivo Using Antimicrobial AgentsJen PanganibanNo ratings yet
- Microbio LEC SAS 1Document3 pagesMicrobio LEC SAS 1spooderm4nNo ratings yet
- Yaws UphDocument44 pagesYaws UphJoshua ObrienNo ratings yet
- Roundworm: Amor B. TalotaloDocument1 pageRoundworm: Amor B. TalotaloRodrigoNo ratings yet
- Jurnal Diare RotavirusDocument6 pagesJurnal Diare RotavirusAnhi RamdhaniNo ratings yet
- FtsequencebraceletsDocument6 pagesFtsequencebraceletsapi-312168736No ratings yet
- ENT Lectures 1Document123 pagesENT Lectures 1lxnalexander100% (1)
- MastoiditisDocument5 pagesMastoiditisJessica Fredelina0% (1)