You might also like
- Pulmonary Assessment and Management of Patients with Pediatric Neuromuscular DiseaseFrom EverandPulmonary Assessment and Management of Patients with Pediatric Neuromuscular DiseaseOscar Henry MayerNo ratings yet
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareFrom EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNo ratings yet
- Effectiveness of Chest Physical Therapy in Improving Quality of Life and Reducing Patient Hospital Stay in Chronic Obstructive Pulmonary DiseaseDocument5 pagesEffectiveness of Chest Physical Therapy in Improving Quality of Life and Reducing Patient Hospital Stay in Chronic Obstructive Pulmonary DiseaseAn O NimNo ratings yet
- Effects of Lung Expansion Therapy On Lung Function in Patients With Prolonged Mechanical VentilationDocument7 pagesEffects of Lung Expansion Therapy On Lung Function in Patients With Prolonged Mechanical Ventilationcard breatheNo ratings yet
- 37 Iajps37112017 PDFDocument4 pages37 Iajps37112017 PDFBaru Chandrasekhar RaoNo ratings yet
- Research Proposal: MPT (Cardio Respiratory Disorders)Document14 pagesResearch Proposal: MPT (Cardio Respiratory Disorders)permanaNo ratings yet
- Pakistan DyspneaDocument7 pagesPakistan DyspneaNelson LoboNo ratings yet
- Proforma For Registration of Subjects For DissertationDocument16 pagesProforma For Registration of Subjects For DissertationAldrich MabasaNo ratings yet
- Reviews: The Effect of Incentive Spirometry On Postoperative Pulmonary ComplicationsDocument8 pagesReviews: The Effect of Incentive Spirometry On Postoperative Pulmonary ComplicationsCENTRO MEDICO ADOLFO LOPEZ MATEOSNo ratings yet
- PTC 2019 0025Document13 pagesPTC 2019 0025archivelalaaNo ratings yet
- Research Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailureDocument7 pagesResearch Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailurewiwiNo ratings yet
- Teknik Acbt Untuk Kasus BronkhiektasisDocument9 pagesTeknik Acbt Untuk Kasus Bronkhiektasisfister19 rifaudinNo ratings yet
- For The Partial Fulfilment of The Degree Of: ABDUL HAMEED (Student of DPT)Document15 pagesFor The Partial Fulfilment of The Degree Of: ABDUL HAMEED (Student of DPT)SheiKh FaiZanNo ratings yet
- Jurnal 5Document7 pagesJurnal 5nskhldNo ratings yet
- Deep Breathing Exercise Education Receiving and Performing Status of Patients Undergoing Abdominal SurgeryDocument4 pagesDeep Breathing Exercise Education Receiving and Performing Status of Patients Undergoing Abdominal SurgeryRianNo ratings yet
- Effectiveness of Diaphragmatic Stretching Versus Rib Stretching On Improving Pulmonary Function and Thoracic Excursion in Subjects With COPDDocument9 pagesEffectiveness of Diaphragmatic Stretching Versus Rib Stretching On Improving Pulmonary Function and Thoracic Excursion in Subjects With COPDInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Autogenic 1 PDFDocument5 pagesAutogenic 1 PDFpermanaNo ratings yet
- DFHDF DFJKJK DFDocument8 pagesDFHDF DFJKJK DFAndrés Araneda VásquezNo ratings yet
- Nair 2019Document8 pagesNair 2019Anonymous VjiuWvATgNo ratings yet
- Endurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsDocument6 pagesEndurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsMuhammad RedhaNo ratings yet
- Clinical Study: What Is The Best Pulmonary Physiotherapy Method in ICU?Document5 pagesClinical Study: What Is The Best Pulmonary Physiotherapy Method in ICU?Sofranita Ladyas PutriNo ratings yet
- The Effectiveness of Pre-Operative Deep BreathingDocument5 pagesThe Effectiveness of Pre-Operative Deep BreathingJulenda CintarinovaNo ratings yet
- Wang 2022Document11 pagesWang 2022Carlos Daniel AliagaNo ratings yet
- Endurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsDocument6 pagesEndurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsMuhammad RedhaNo ratings yet
- 10.1038@s41390 020 0874 XDocument9 pages10.1038@s41390 020 0874 Xhabib diopNo ratings yet
- 22 Effect of Incentive Spirometer Exercise On Pulmonary Functions in Children With Spastic Cerebral PalsyDocument6 pages22 Effect of Incentive Spirometer Exercise On Pulmonary Functions in Children With Spastic Cerebral PalsyDoaa TammamNo ratings yet
- Nirali Final Synopsis PDFDocument31 pagesNirali Final Synopsis PDFNIRALI MISTRYNo ratings yet
- Heart & Lung: Care of Critically Ill AdultsDocument13 pagesHeart & Lung: Care of Critically Ill AdultsRabiyatul AwaliyahNo ratings yet
- Avances en Terapia de Rehabilitacion CardiopulmonarDocument13 pagesAvances en Terapia de Rehabilitacion CardiopulmonarMaría Camila Zuluaga AriasNo ratings yet
- Indian Journal of Nursing SciencesDocument5 pagesIndian Journal of Nursing Sciencesmadhu.BNo ratings yet
- MainDocument10 pagesMainMu RakimNo ratings yet
- Chest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Document19 pagesChest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Physio EbookNo ratings yet
- Paper Epoc PDFDocument5 pagesPaper Epoc PDFNicolás Celis MonroyNo ratings yet
- Efficacy of Interventions To Improve Respiratory Function After StrokeDocument14 pagesEfficacy of Interventions To Improve Respiratory Function After StrokeagstriansNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, Karnataka Proforma For Registration of Subjects For DissertationDocument12 pagesRajiv Gandhi University of Health Sciences Bangalore, Karnataka Proforma For Registration of Subjects For DissertationyashramawatNo ratings yet
- Role of Spirometry in Post CABG PtsDocument11 pagesRole of Spirometry in Post CABG PtsBeshoy KhelaNo ratings yet
- Aerobic Training On Dyspnea Chest Wall CopdDocument8 pagesAerobic Training On Dyspnea Chest Wall CopdBunga Mitra MampuNo ratings yet
- Articulo Effect of Flashlight Guidance On Manual Ventilation Performance in Cardiopulmonary Resuscitation A Randomized Controlled Simulation StudyDocument11 pagesArticulo Effect of Flashlight Guidance On Manual Ventilation Performance in Cardiopulmonary Resuscitation A Randomized Controlled Simulation StudyCindy Katherine LlanosNo ratings yet
- Exploring A Physiotherapy Well-Being Review To Deliver Community-Based Rehabilitation in Patients With Pulmonary HypertensionDocument9 pagesExploring A Physiotherapy Well-Being Review To Deliver Community-Based Rehabilitation in Patients With Pulmonary HypertensionPaulomds1991No ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document8 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Research ParkNo ratings yet
- JCDR 10 KC01 PDFDocument6 pagesJCDR 10 KC01 PDFaarti sharmaNo ratings yet
- Clinical Respiratory J - 2018 - Beaumont - Effects of Inspiratory Muscle Training in COPD Patients A Systematic Review andDocument11 pagesClinical Respiratory J - 2018 - Beaumont - Effects of Inspiratory Muscle Training in COPD Patients A Systematic Review andAlejandra Castro BelloNo ratings yet
- Desmame ProlongadoDocument7 pagesDesmame ProlongadoAssessoria da Gerência Geral HEHANo ratings yet
- Chatham 2004Document5 pagesChatham 2004raul huertaNo ratings yet
- Effects of Combined Aerobic Strength Training Versus Fitness Education Program in CopdDocument9 pagesEffects of Combined Aerobic Strength Training Versus Fitness Education Program in Copdsana manzoorNo ratings yet
- 348-Article Text-1233-1-10-20201221Document5 pages348-Article Text-1233-1-10-20201221Salsabila FitriaNo ratings yet
- BMJ Open 2015 ZhangDocument10 pagesBMJ Open 2015 ZhangLuis CordovaNo ratings yet
- Severgnini 2013Document15 pagesSevergnini 2013moraeunwprqphslndfNo ratings yet
- Driving Pressure Study OLVDocument13 pagesDriving Pressure Study OLVlucasNo ratings yet
- CF Ventilation ManagementDocument10 pagesCF Ventilation ManagementSherry SaidNo ratings yet
- Early Mobilization To Prevent AtelectasisDocument6 pagesEarly Mobilization To Prevent AtelectasisLucia NatashaNo ratings yet
- Journal Bedah Thorax 2Document15 pagesJournal Bedah Thorax 2Novia LarasatiNo ratings yet
- Artículo PulmonarDocument9 pagesArtículo PulmonarSamuel GasparNo ratings yet
- Pjms 32 1152Document6 pagesPjms 32 1152api-459288956No ratings yet
- Physiotherapy in The ICUDocument10 pagesPhysiotherapy in The ICUakheel ahammedNo ratings yet
- 1 s2.0 S2531043718301107 MainDocument8 pages1 s2.0 S2531043718301107 MainCraniolyne RefianNo ratings yet
- Airway Clearance TherapiesDocument12 pagesAirway Clearance TherapiesMiguelandry PérezNo ratings yet
- Comparative Study of Breathing Techniques After Coronary Artery by Pass GraftingDocument12 pagesComparative Study of Breathing Techniques After Coronary Artery by Pass GraftingJulenda CintarinovaNo ratings yet
- KTR Tecnica EvidenciaDocument12 pagesKTR Tecnica EvidenciacarlitrossotoNo ratings yet
- Fisioterapia en La UCI - William Cristancho Gómez - 231019 - 183432Document24 pagesFisioterapia en La UCI - William Cristancho Gómez - 231019 - 183432Ale SanchezNo ratings yet
- University Students 2Document2 pagesUniversity Students 2احمد العايديNo ratings yet
- Research Article: Clinical Decision Making of Nurses Working in Hospital SettingsDocument8 pagesResearch Article: Clinical Decision Making of Nurses Working in Hospital Settingsاحمد العايديNo ratings yet
- Knowledge and Perception of The Employees S Towards COVID-19 Vaccination at Palestinian UniversitiesDocument6 pagesKnowledge and Perception of The Employees S Towards COVID-19 Vaccination at Palestinian Universitiesاحمد العايديNo ratings yet
- Psychological Reactions of Lebanese Nurses To Workplace Violence in Critical Care UnitsDocument13 pagesPsychological Reactions of Lebanese Nurses To Workplace Violence in Critical Care Unitsاحمد العايديNo ratings yet
- Nursing Informatics Competency and Self Efficacy in Clinical Practice Among Nurses in Palestinian Hospitals-2Document1 pageNursing Informatics Competency and Self Efficacy in Clinical Practice Among Nurses in Palestinian Hospitals-2احمد العايديNo ratings yet
- The Effect of Computer-Based Tests On Nursing Students' Test Anxiety: A Quasi-Experimental StudyDocument4 pagesThe Effect of Computer-Based Tests On Nursing Students' Test Anxiety: A Quasi-Experimental Studyاحمد العايديNo ratings yet
- University Students 3Document2 pagesUniversity Students 3احمد العايديNo ratings yet
- Sources of Stress and Coping Behaviors Among Nursing Students Throughout Their First Clinical TrainingDocument7 pagesSources of Stress and Coping Behaviors Among Nursing Students Throughout Their First Clinical Trainingاحمد العايديNo ratings yet
- Correlation Between Anthropometric MeasurementsDocument11 pagesCorrelation Between Anthropometric Measurementsاحمد العايديNo ratings yet
- Delirium in Intensive Care Units Perceptions Of.6Document10 pagesDelirium in Intensive Care Units Perceptions Of.6احمد العايديNo ratings yet
- The Impacts of Emerging Pollutants On Human Health and EnvironmentDocument12 pagesThe Impacts of Emerging Pollutants On Human Health and Environmentاحمد العايديNo ratings yet
- Effectiveness of StretchingDocument10 pagesEffectiveness of Stretchingاحمد العايديNo ratings yet
- The Relationship Between Stress and Resilience of Nurses in Intensive Care Units During COVID19Document8 pagesThe Relationship Between Stress and Resilience of Nurses in Intensive Care Units During COVID19احمد العايديNo ratings yet
- The Impacts of Emerging Pollutants On Human Health and EnvironmentDocument12 pagesThe Impacts of Emerging Pollutants On Human Health and Environmentاحمد العايديNo ratings yet
- Predictors of HypertensionDocument5 pagesPredictors of Hypertensionاحمد العايديNo ratings yet
- Stress and Coping Among PT StudentsDocument6 pagesStress and Coping Among PT Studentsاحمد العايديNo ratings yet
- Nurse's Perception of Barriers To Research 2020Document14 pagesNurse's Perception of Barriers To Research 2020احمد العايديNo ratings yet
- The Impact of Concept Mapping On CaringDocument9 pagesThe Impact of Concept Mapping On Caringاحمد العايديNo ratings yet
- A Descriptive Cross-Sectional Study To AssessDocument10 pagesA Descriptive Cross-Sectional Study To Assessاحمد العايديNo ratings yet
- Delirium in Intensive Care Units Perceptions Of.6Document10 pagesDelirium in Intensive Care Units Perceptions Of.6احمد العايديNo ratings yet
- Health-Promoting Behaviors Among NursingDocument5 pagesHealth-Promoting Behaviors Among Nursingاحمد العايديNo ratings yet
- Impact of Night Shift and Training Development Factors OnDocument12 pagesImpact of Night Shift and Training Development Factors Onاحمد العايديNo ratings yet
- Comparative Assessment of Basic Life Support KnowledgeDocument5 pagesComparative Assessment of Basic Life Support Knowledgeاحمد العايديNo ratings yet
- Breast Self-Examination in Terms of Knowledge, Attitude, andDocument12 pagesBreast Self-Examination in Terms of Knowledge, Attitude, andSameer Ahmad100% (1)
- Core Measure: 10 Meter Walk Test (10mWT) : Pace and Stop When You Reach The Far Mark."Document6 pagesCore Measure: 10 Meter Walk Test (10mWT) : Pace and Stop When You Reach The Far Mark."احمد العايديNo ratings yet
- Are Standard Precautions For Hospital Acquired InfectionDocument5 pagesAre Standard Precautions For Hospital Acquired Infectionاحمد العايديNo ratings yet
- Midwives and Nurses Compliance WithDocument9 pagesMidwives and Nurses Compliance Withاحمد العايديNo ratings yet
- The Outcomes of Integrating High FidelityDocument11 pagesThe Outcomes of Integrating High Fidelityاحمد العايديNo ratings yet
- Clinical StudyDocument8 pagesClinical Studyاحمد العايديNo ratings yet
- Gait & Posture: SciencedirectDocument8 pagesGait & Posture: Sciencedirectاحمد العايديNo ratings yet
- As 2419Document93 pagesAs 2419Craftychemist100% (2)
- Laser Pointing StabilityDocument5 pagesLaser Pointing Stabilitymehdi810No ratings yet
- Pro & Contra Hydropower: AdvantagesDocument16 pagesPro & Contra Hydropower: AdvantagesbarukomkssNo ratings yet
- Oman Vision 2040 Vision Document 8Document27 pagesOman Vision 2040 Vision Document 8Abdul Aziz AlbalushiNo ratings yet
- Project - PPT 5 ImplementationDocument39 pagesProject - PPT 5 ImplementationBirhanu AbrhaNo ratings yet
- SWP-10 Loading & Unloading Using Lorry & Mobile Crane DaimanDocument2 pagesSWP-10 Loading & Unloading Using Lorry & Mobile Crane DaimanHassan AbdullahNo ratings yet
- GTA Liberty City Stories CheatsDocument6 pagesGTA Liberty City Stories CheatsHubbak KhanNo ratings yet
- IoscanDocument3 pagesIoscanTimNo ratings yet
- Industrial Disputes Act1947 Cases: By: Anil Ashish Topno ROLL NO: 12003 Retail Management 2 YearDocument15 pagesIndustrial Disputes Act1947 Cases: By: Anil Ashish Topno ROLL NO: 12003 Retail Management 2 YearAnil Ashish Topno100% (1)
- Affidavit of WaiverDocument1 pageAffidavit of Waivergelbert palomarNo ratings yet
- Satyam GargDocument2 pagesSatyam GargSatyam GargNo ratings yet
- Casio fx-82MSDocument49 pagesCasio fx-82MSPéter GedeNo ratings yet
- Ordinary Differential Equations Multiple Choice Questions and Answers - SanfoundryDocument7 pagesOrdinary Differential Equations Multiple Choice Questions and Answers - SanfoundrySaiman PervaizNo ratings yet
- Yrc1000 Options InstructionsDocument36 pagesYrc1000 Options Instructionshanh nguyenNo ratings yet
- Purposeful InnovationDocument6 pagesPurposeful InnovationKeith Tanaka MagakaNo ratings yet
- Section 2 Structure and FunctionDocument42 pagesSection 2 Structure and FunctionRached Douahchua100% (1)
- Suite Popular Brasileira: 5. Shorinho Heitor Villa-LobosDocument4 pagesSuite Popular Brasileira: 5. Shorinho Heitor Villa-Loboshuong trinhNo ratings yet
- EE 4702 Take-Home Pre-Final Questions: SolutionDocument11 pagesEE 4702 Take-Home Pre-Final Questions: SolutionmoienNo ratings yet
- Motion For Forensic Examination - Cyber CasedocxDocument5 pagesMotion For Forensic Examination - Cyber CasedocxJazz Tracey100% (1)
- Vanderbeck Solman ch01-10Document156 pagesVanderbeck Solman ch01-10Jelly AceNo ratings yet
- Vehicle To Vehicle V2V Communication Scope Importa PDFDocument13 pagesVehicle To Vehicle V2V Communication Scope Importa PDFvahidinkormanNo ratings yet
- FAC1502 Bank Reconcilliation NotesDocument22 pagesFAC1502 Bank Reconcilliation NotesMichelle Foord0% (1)
- Local Training Companies DBDocument8 pagesLocal Training Companies DBMohammad MuhannaNo ratings yet
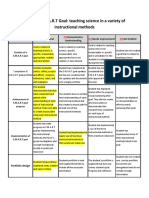
- Smart Goals Rubric 2Document2 pagesSmart Goals Rubric 2api-338549230100% (2)
- VDO Gauge - VL Hourmeter 12 - 24Document2 pagesVDO Gauge - VL Hourmeter 12 - 24HanNo ratings yet
- Pre Int Work Book Unit 9Document8 pagesPre Int Work Book Unit 9Maria Andreina Diaz SantanaNo ratings yet
- Milling of Legume PulsesDocument7 pagesMilling of Legume Pulsessuresh100% (1)
- Bc-6800plus Series Auto Hematology Analyzer Operator's ManualDocument322 pagesBc-6800plus Series Auto Hematology Analyzer Operator's ManualHenock MelesseNo ratings yet
- CPS Fitting Stations by County - 22 - 0817Document33 pagesCPS Fitting Stations by County - 22 - 0817Melissa R.No ratings yet
- Rai Work Experience SheetDocument2 pagesRai Work Experience Sheetmark langcayNo ratings yet