You might also like
- Medical Conditions Associated with Suicide Risk: Suicide and Dysmetabolisms: A Focus on ProlactinFrom EverandMedical Conditions Associated with Suicide Risk: Suicide and Dysmetabolisms: A Focus on ProlactinNo ratings yet
- Suicide Risk Assessment and Prevention. Challenges and OpportunitiesDocument12 pagesSuicide Risk Assessment and Prevention. Challenges and OpportunitiesMaira Espinoza LabraNo ratings yet
- Medical Conditions Associated with Suicide Risk: Suicide and Migraines and Chronic HeadachesFrom EverandMedical Conditions Associated with Suicide Risk: Suicide and Migraines and Chronic HeadachesNo ratings yet
- Estrategias de Prevención de Suicidio JAMADocument11 pagesEstrategias de Prevención de Suicidio JAMAapi-26621755No ratings yet
- Medical Conditions Associated with Suicide Risk: Suicidal Risk in Patients with Diabetes MellitusFrom EverandMedical Conditions Associated with Suicide Risk: Suicidal Risk in Patients with Diabetes MellitusNo ratings yet
- Improving Suicide Prevention Evidenced Based Strategies 2021Document26 pagesImproving Suicide Prevention Evidenced Based Strategies 2021NeuroArmonia KidsNo ratings yet
- Goldman-Mellor Et Al 2014 Suicide Attempt in Young People - A Signal For Long-Term Health Care and Social NeedsDocument9 pagesGoldman-Mellor Et Al 2014 Suicide Attempt in Young People - A Signal For Long-Term Health Care and Social NeedsAdam OsborneNo ratings yet
- Demographic and Clinical Correlates of Suicidality in Adolescents Attending A Specialist Community Mental Health Service: A Naturalistic StudyDocument6 pagesDemographic and Clinical Correlates of Suicidality in Adolescents Attending A Specialist Community Mental Health Service: A Naturalistic StudyAna Paula Soares GondimNo ratings yet
- Mental Health Problems and Risk of Suicidal Ideation and Attempts in AdolescentDocument10 pagesMental Health Problems and Risk of Suicidal Ideation and Attempts in AdolescentFlóra FarkasNo ratings yet
- A Meta-Analysis of Neuropsychological Markers of Vulnerability To Suicidal Behavior in Mood DisordersDocument12 pagesA Meta-Analysis of Neuropsychological Markers of Vulnerability To Suicidal Behavior in Mood DisordersWALTER DE PAZNo ratings yet
- Mann Alapter Bertolote Et Al - Suicide Prevention Strategies-Systematic ReviewDocument12 pagesMann Alapter Bertolote Et Al - Suicide Prevention Strategies-Systematic ReviewAnna MaryaNo ratings yet
- N 509 MaterialsDocument128 pagesN 509 MaterialsgdomagasNo ratings yet
- 1 s2.0 S2666354620300892 MainDocument11 pages1 s2.0 S2666354620300892 MainMaría Camila Trujillo LópezNo ratings yet
- The Role of Negative Affect and Self-Concept Clarity in Predicting Self-Injurious Urges in Borderline Personality Disorder Using Ecological Momentary AssessmentDocument22 pagesThe Role of Negative Affect and Self-Concept Clarity in Predicting Self-Injurious Urges in Borderline Personality Disorder Using Ecological Momentary Assessmentme13No ratings yet
- HHS Public AccessDocument25 pagesHHS Public AccessIohanny de Oliveira BarbosaNo ratings yet
- Article - Mental Disorders, Comorbidities, and Suicidality at 30 Years BrazilDocument9 pagesArticle - Mental Disorders, Comorbidities, and Suicidality at 30 Years BrazilRafael Iwamoto TosiNo ratings yet
- Crisis SuicidioDocument10 pagesCrisis SuicidioMaitte Carrión UribeNo ratings yet
- Pi Is 2215036614702573Document3 pagesPi Is 2215036614702573RealAelixirNo ratings yet
- Seminar: Gustavo Turecki, David A BrentDocument13 pagesSeminar: Gustavo Turecki, David A BrentamaliamldNo ratings yet
- 9.the Role of Inflammation in Suicidal BehaviourDocument12 pages9.the Role of Inflammation in Suicidal BehaviourWendy QuintanaNo ratings yet
- (Art) 2005 - Complicated Grief and Suicidal Ideation in Adult Survivors of SuicideDocument9 pages(Art) 2005 - Complicated Grief and Suicidal Ideation in Adult Survivors of SuicideAyúdate Con PsicologíaNo ratings yet
- Suicide Prevention in Psychiatric PatientsDocument11 pagesSuicide Prevention in Psychiatric PatientsDaniela DiazNo ratings yet
- BJP 2018 27Document8 pagesBJP 2018 27Manon MorenoNo ratings yet
- Artigo (Inglês) Acute Risk Factors For Suicide Attempts and Death - Prospective Findings From The STEP-BD StudyDocument19 pagesArtigo (Inglês) Acute Risk Factors For Suicide Attempts and Death - Prospective Findings From The STEP-BD StudyIohanny de Oliveira BarbosaNo ratings yet
- Lombardo - New Frontiers in Suicide Vulnerability Immune System and Sex Hormones - 2021Document8 pagesLombardo - New Frontiers in Suicide Vulnerability Immune System and Sex Hormones - 2021dojabrNo ratings yet
- Psychotic Symptoms and Population Risk For Suicide Attempt A Prospective Cohort StudyDocument9 pagesPsychotic Symptoms and Population Risk For Suicide Attempt A Prospective Cohort StudyGiselle Andrea Naranjo VillateNo ratings yet
- Bipolar Disorders - 2022 - DimickDocument2 pagesBipolar Disorders - 2022 - DimickDaniela Pia VelosoNo ratings yet
- Professional Adversities and Protective Factors Associated With Suicidal Ideation in Mexican PsychiatristsDocument6 pagesProfessional Adversities and Protective Factors Associated With Suicidal Ideation in Mexican Psychiatristssamsoto86No ratings yet
- Risk Factors Associated With Psychiatric Comorbidities Among Suicide AttemptersDocument8 pagesRisk Factors Associated With Psychiatric Comorbidities Among Suicide AttemptersSteve aokiNo ratings yet
- Introduction For Suicide Study 2167 0943 1000227Document4 pagesIntroduction For Suicide Study 2167 0943 1000227wilsonidongesit072No ratings yet
- Stanleyetal.2016 TheoriesofSuicide OlderAdultsDocument10 pagesStanleyetal.2016 TheoriesofSuicide OlderAdultsSharvari ShahNo ratings yet
- Neuropsicologia Conducta SuicidaDocument12 pagesNeuropsicologia Conducta SuicidaFanny FrEgosoNo ratings yet
- Risk Factors For Fatal and Nonfatal Repetition of Suicide Attempts: A Literature ReviewDocument12 pagesRisk Factors For Fatal and Nonfatal Repetition of Suicide Attempts: A Literature ReviewMuhammad AdithiaNo ratings yet
- Research On The Pathophysiology, Treatment, and Prevention of Suicide: Practical and Ethical IssuesDocument12 pagesResearch On The Pathophysiology, Treatment, and Prevention of Suicide: Practical and Ethical IssuesIsuru TharakaNo ratings yet
- Evaluation of The Quality of Life and Risk of Suicide: Clinical ScienceDocument5 pagesEvaluation of The Quality of Life and Risk of Suicide: Clinical ScienceMinodora MilenaNo ratings yet
- Suicidal Ideation - StatPearls - NCBI BookshelfDocument13 pagesSuicidal Ideation - StatPearls - NCBI BookshelfRicardo EscNo ratings yet
- Literature Review of Suicide in Cancer PatientsDocument5 pagesLiterature Review of Suicide in Cancer Patientsafdtzvbex100% (1)
- 05 Ijpscr 125 23Document12 pages05 Ijpscr 125 23BRNSS Publication Hub InfoNo ratings yet
- fpubh-12-1372974Document15 pagesfpubh-12-1372974sosfudanfengNo ratings yet
- Evaluation of Suicidal Patients - The SAD PERSONS ScaleDocument5 pagesEvaluation of Suicidal Patients - The SAD PERSONS ScaleCecilia GuzmánNo ratings yet
- Disease Primers, 5, 74. (Doi:: Enlighten - Research Publications by Members of The University of GlasgowDocument51 pagesDisease Primers, 5, 74. (Doi:: Enlighten - Research Publications by Members of The University of GlasgowTrade TechnologiesNo ratings yet
- 35 Years Suicidal PatientsDocument70 pages35 Years Suicidal PatientsAnonymous kJxwzJglNo ratings yet
- Journal Reading DennyDocument14 pagesJournal Reading DennyDenny EmiliusNo ratings yet
- Prevalence of Suicide Attempts in Bipolar Disorder A Systematic Review and Meta Analysis of Observational StudiesDocument9 pagesPrevalence of Suicide Attempts in Bipolar Disorder A Systematic Review and Meta Analysis of Observational StudiesislameoaNo ratings yet
- An Evidence-Based Approach To Evaluating and Managing Suicidal EmergenciesDocument22 pagesAn Evidence-Based Approach To Evaluating and Managing Suicidal EmergencieslorainecumplidoNo ratings yet
- Psychology and Suicidal ThoughtsDocument10 pagesPsychology and Suicidal ThoughtsMark MansonNo ratings yet
- Changing Global Face of SuicideDocument2 pagesChanging Global Face of SuicideDinesh KumarNo ratings yet
- Tide Malm 2014Document9 pagesTide Malm 2014opanocayNo ratings yet
- Prevention of Suicidal Behavior in Older PeopleDocument14 pagesPrevention of Suicidal Behavior in Older PeopleAndres Felipe Arias OrtizNo ratings yet
- Exploring The Risk Factors of Suicide AttemptersDocument25 pagesExploring The Risk Factors of Suicide AttemptersDrkhalidaraufgmail.com RAUFNo ratings yet
- Adolescent Suicides...... 12Document6 pagesAdolescent Suicides...... 12William OtienoNo ratings yet
- McCauley, Linehan, 2018Document9 pagesMcCauley, Linehan, 2018jesusNo ratings yet
- Suicidal Ideation - StatPearls - NCBI BookshelfDocument35 pagesSuicidal Ideation - StatPearls - NCBI BookshelfJan LAWNo ratings yet
- fpubh-11-1097098Document11 pagesfpubh-11-1097098tafazzal.eduNo ratings yet
- Prevalence and Correlates of Suicide Planning and Attempt Among Individuals With SIDocument8 pagesPrevalence and Correlates of Suicide Planning and Attempt Among Individuals With SIIsaac FullartonNo ratings yet
- Suicide in The ElderlyDocument8 pagesSuicide in The ElderlyCRISTIAN VALERONo ratings yet
- Div Class Title Psychosocial Factors That Distinguish Between Men and Women Who Have Suicidal Thoughts and Attempt Suicide Findings From a National Probability Sample of Adults DivDocument9 pagesDiv Class Title Psychosocial Factors That Distinguish Between Men and Women Who Have Suicidal Thoughts and Attempt Suicide Findings From a National Probability Sample of Adults Divsachinkuk6196No ratings yet
- Content ServerDocument32 pagesContent ServerNatalia Alva ZavalaNo ratings yet
- Mehu258 - U8 - T27 - Articulo 2 - Emergencias y Ugencias PsiquiatricasDocument2 pagesMehu258 - U8 - T27 - Articulo 2 - Emergencias y Ugencias PsiquiatricasMaxNo ratings yet
- Efficacy of Dialectical Behavior Therapy For Adolescents at High Risk For SuicideDocument9 pagesEfficacy of Dialectical Behavior Therapy For Adolescents at High Risk For SuicideMartinaNo ratings yet
- PTSDDocument8 pagesPTSDasma khalidNo ratings yet
- Psychology Magazine Issue1 23Document24 pagesPsychology Magazine Issue1 23Marisu Campo-RedondoNo ratings yet
- 2022 23 Mental Health Awareness ToolkitDocument182 pages2022 23 Mental Health Awareness ToolkitCraig MongerNo ratings yet
- Baas Et Al., (2017)Document12 pagesBaas Et Al., (2017)Andrea BarrosoNo ratings yet
- Stop Caretaking The BorderlineDocument1 pageStop Caretaking The Borderlineanca hNo ratings yet
- All Chapter 1Document3 pagesAll Chapter 1Jeselle Faith DuqueNo ratings yet
- PsychiatryDocument13 pagesPsychiatryDr. Hem Sagar GautamNo ratings yet
- Text News AnchorDocument2 pagesText News AnchorPUTRI SHIFA AULIANo ratings yet
- PATHOPHYSIOLOGYDocument1 pagePATHOPHYSIOLOGYJhexy Rhay BayagenNo ratings yet
- 10 Things About CodependencyDocument3 pages10 Things About CodependencyAsmaa El-emairy100% (1)
- Jurnal SafiraDocument5 pagesJurnal SafiraAliva AzzahraNo ratings yet
- NCP TikDocument4 pagesNCP Tikblancher erNo ratings yet
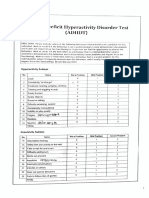
- Attention Deficit Hyperactivity Disorder TestDocument6 pagesAttention Deficit Hyperactivity Disorder Testmehna nawasNo ratings yet
- FINAL AED Purple Nutrition Book RemovedDocument28 pagesFINAL AED Purple Nutrition Book RemovedOla Conde VIINo ratings yet
- Abnormal Psychology in A Changing World 10th Edition Nevid Solutions Manual DownloadDocument13 pagesAbnormal Psychology in A Changing World 10th Edition Nevid Solutions Manual DownloadMelinda Smith100% (25)
- DSM 5 TR DrukDocument14 pagesDSM 5 TR Drukmalami34No ratings yet
- Unit Plan - Psychology 12Document5 pagesUnit Plan - Psychology 12api-639942719No ratings yet
- Original PDF Psychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice 9th PDFDocument41 pagesOriginal PDF Psychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice 9th PDFjoseph.owens578100% (36)
- Dissociative, Somatic and Sleep DisordersDocument38 pagesDissociative, Somatic and Sleep DisordersNatalya CespedesNo ratings yet
- Abnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual 1Document21 pagesAbnormal Psychology Plus NEW MyPsychLab 15th Edition Butcher Solutions Manual 1william100% (39)
- Case Study For MDDDocument9 pagesCase Study For MDDifatimanaqvi1472No ratings yet
- Sample Case StudyDocument5 pagesSample Case StudyAntonia AmpireNo ratings yet
- Personality Disorders PDFDocument19 pagesPersonality Disorders PDFrurban manipurNo ratings yet
- Obsessive-Compulsive Disorder - StatPearls - NCBI BookshelfDocument7 pagesObsessive-Compulsive Disorder - StatPearls - NCBI BookshelfDhany karubuyNo ratings yet
- Dialectical Behaviour Therapy - Theoretical Principles and StrategiesDocument17 pagesDialectical Behaviour Therapy - Theoretical Principles and StrategiesYudhajit RoychowdhuryNo ratings yet
- Concept PaperDocument2 pagesConcept PaperLea May VillajuanNo ratings yet
- People VS Haloc Case DigestDocument2 pagesPeople VS Haloc Case DigestHannah HazelNo ratings yet
- Othello Syndrome: Its Effect On Family RelationshipDocument24 pagesOthello Syndrome: Its Effect On Family RelationshipNICHOLAS CLEMENTNo ratings yet
- CBT and Internet GamingDocument13 pagesCBT and Internet Gamingkafi naNo ratings yet
- Suicide Risk Assessment Template UpdatedDocument3 pagesSuicide Risk Assessment Template UpdatedZhillNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessFrom EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessRating: 5 out of 5 stars5/5 (6)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Triggers: How We Can Stop Reacting and Start HealingFrom EverandTriggers: How We Can Stop Reacting and Start HealingRating: 5 out of 5 stars5/5 (58)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1244)
- Embrace Your Weird: Face Your Fears and Unleash CreativityFrom EverandEmbrace Your Weird: Face Your Fears and Unleash CreativityRating: 4.5 out of 5 stars4.5/5 (124)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- The Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.From EverandThe Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.Rating: 5 out of 5 stars5/5 (14)
- Are You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersFrom EverandAre You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersRating: 5 out of 5 stars5/5 (29)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)