You might also like
- eSCAPE by Anik Singal PDFDocument444 pageseSCAPE by Anik Singal PDFᜎᜒᜐ᜔ᜆᜒᜇ᜔ ᜎᜋ᜔ᜊᜒᜇ᜔ᜆᜒ ᜂᜐᜉ᜔ᜇᜒᜈ᜔100% (20)
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- FM-CSVlrd-01 S2 Application Rev 0 April 30 2018 02AUG2018Document2 pagesFM-CSVlrd-01 S2 Application Rev 0 April 30 2018 02AUG2018Noel IV T. Borromeo50% (4)
- Philippine Drug Enforcement Agency: S1 S3 S4 S5C S5D S5-E S5-I S6Document2 pagesPhilippine Drug Enforcement Agency: S1 S3 S4 S5C S5D S5-E S5-I S6Sherwin Ugdamin100% (1)
- Change Management AssignmentDocument7 pagesChange Management AssignmentMfaeez Fiz50% (2)
- Report To The Mississippi Charter School Authorizer Board 2014 - 2022 Charter School Application CycleDocument11 pagesReport To The Mississippi Charter School Authorizer Board 2014 - 2022 Charter School Application CycleRuss LatinoNo ratings yet
- AaaaaaDocument2 pagesAaaaaaUltra FreshNo ratings yet
- s2 ApplicationDocument2 pagess2 ApplicationIze MarieNo ratings yet
- Pdea Form 2024Document2 pagesPdea Form 2024Digos Doctors' Hospital, Inc. IT DepartmentNo ratings yet
- Pdea - S-License Application Form 2023Document2 pagesPdea - S-License Application Form 2023Arnel Lajo FulgencioNo ratings yet
- ContentDocument1 pageContentST ANNE GENERAL HOSPITAL INC (SAFETY DEPARTMENT)No ratings yet
- s2 ApplicDocument1 pages2 ApplicArnel Lajo FulgencioNo ratings yet
- PSC Application Form (Non-Registered) - Doctor BagjaDocument7 pagesPSC Application Form (Non-Registered) - Doctor BagjaAnita AjNo ratings yet
- Arcega Maria Lucia R. 3 15 24 RevisedDocument1 pageArcega Maria Lucia R. 3 15 24 RevisedMark BaniagaNo ratings yet
- Arcega Florence Diane R. 3 15 24. RevisedDocument1 pageArcega Florence Diane R. 3 15 24. RevisedMark BaniagaNo ratings yet
- Arcega Arnel S. 3 15 24. RevisedDocument1 pageArcega Arnel S. 3 15 24. RevisedMark BaniagaNo ratings yet
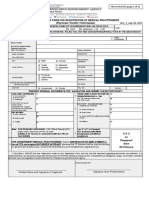
- S2 Application Form For Registration of Medical Practitioners (Physician / Dentist / Veterinarian)Document2 pagesS2 Application Form For Registration of Medical Practitioners (Physician / Dentist / Veterinarian)Gerika Aura RPh0% (1)
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceTEJA SINGHNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceHemantNo ratings yet
- PDR - 03072014 Philhealth Form PDFDocument1 pagePDR - 03072014 Philhealth Form PDFMARY ANGELIE G. MANALANGNo ratings yet
- NFL Recruitment 2022Document6 pagesNFL Recruitment 2022Ghostcscz LaggingNo ratings yet
- L2200167097 - T2200074253 - 2022-161216 - Ramos, Bayani A. - 07072022071443-161216 - 1140 - 0 - 19920509 - $cov-RpttDocument2 pagesL2200167097 - T2200074253 - 2022-161216 - Ramos, Bayani A. - 07072022071443-161216 - 1140 - 0 - 19920509 - $cov-RpttYanz RamsNo ratings yet
- HP Commonwealth (Bartolome, Kendrick)Document1 pageHP Commonwealth (Bartolome, Kendrick)maryjoyloma04No ratings yet
- Form No. 6 Revised 2020 ASDS Meilrose PeraltaDocument2 pagesForm No. 6 Revised 2020 ASDS Meilrose PeraltaYULAINE CARILLONo ratings yet
- Jereco T. Basilio, MD Municipal Health Officer E. Mercado St. Poblacion, Sto. Tomas, PampangaDocument1 pageJereco T. Basilio, MD Municipal Health Officer E. Mercado St. Poblacion, Sto. Tomas, PampangaMARY ANGELIE G. MANALANGNo ratings yet
- Federal Staff Relief Fund FormDocument1 pageFederal Staff Relief Fund Formkazmi_jeNo ratings yet
- Medical Services Division: Hi-Precision Diagnostics (V Luna Branch)Document1 pageMedical Services Division: Hi-Precision Diagnostics (V Luna Branch)Ren RenNo ratings yet
- FM-CSVlrd-02 - S License - Rev - 2 - April 01 2022 - 04apr2022Document2 pagesFM-CSVlrd-02 - S License - Rev - 2 - April 01 2022 - 04apr2022Princess Kate PedrosoNo ratings yet
- Philippine Health Insurance Corporation: Part I - Health Care Institution (Hci) InformationDocument2 pagesPhilippine Health Insurance Corporation: Part I - Health Care Institution (Hci) InformationJoshua Caleb CabreraNo ratings yet
- Application For Registration of Company - A. B. DAWANAU PHARMACY LTDDocument8 pagesApplication For Registration of Company - A. B. DAWANAU PHARMACY LTDAhmed Tijjani TukurNo ratings yet
- WBHS Ipd App Form EmpDocument3 pagesWBHS Ipd App Form EmpSouvik DasNo ratings yet
- Philhealth Application FormDocument5 pagesPhilhealth Application Formjoanne estayoNo ratings yet
- Healthcare Provider Application FormDocument7 pagesHealthcare Provider Application FormBun BunNo ratings yet
- Konsulta PDR CIUDocument1 pageKonsulta PDR CIUOrlando PalomponNo ratings yet
- 2020070118Document8 pages2020070118thambisetty prudhviNo ratings yet
- DOH Ssrs New FormDocument2 pagesDOH Ssrs New FormAlvin GULOYNo ratings yet
- Jugao, TeresitaDocument1 pageJugao, Teresitamobai.li.yuNo ratings yet
- Waqas Khan PDFDocument2 pagesWaqas Khan PDFKoko KhanNo ratings yet
- Domingo O. Ignacio - 3251892000309Document10 pagesDomingo O. Ignacio - 3251892000309Roberto IgnacioNo ratings yet
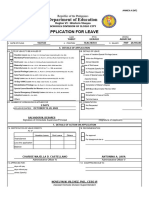
- LEAVE FORM REVISED 2020 For Teacher 5 Days Leave or More - 093623Document2 pagesLEAVE FORM REVISED 2020 For Teacher 5 Days Leave or More - 093623lilibeth padernaNo ratings yet
- Form 6 Revised 2022Document2 pagesForm 6 Revised 2022Angelo AlcantaraNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceVasudevan KunjithapathamNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceHiren PanchalNo ratings yet
- AsaDocument7 pagesAsaAlianna Arnica MambataoNo ratings yet
- San Lazaro Hospital: Republic of The Philippines Department of HealthDocument2 pagesSan Lazaro Hospital: Republic of The Philippines Department of HealthPharmastar Int'l Trading Corp.No ratings yet
- Employee's State Insurance Corporation: Patient RegistrationDocument2 pagesEmployee's State Insurance Corporation: Patient RegistrationafakraipurNo ratings yet
- Amandeep DecDocument2 pagesAmandeep DecUppili Pranavane100% (1)
- Steps and Requirements For QMC POSITIONDocument2 pagesSteps and Requirements For QMC POSITIONCarlos AcuñaNo ratings yet
- Memorandum: Technical Education and Skills Development Authority ISODocument6 pagesMemorandum: Technical Education and Skills Development Authority ISOJe-ann H. GonzalesNo ratings yet
- Shire Cares Application EnglishDocument4 pagesShire Cares Application EnglishDallas PaceNo ratings yet
- 8000100608762655-65083371-Form FDocument1 page8000100608762655-65083371-Form FSinar DuniaNo ratings yet
- RACHEL ANNE VALERIANOJanuary 17 2023-Letter of AuthorizationDocument1 pageRACHEL ANNE VALERIANOJanuary 17 2023-Letter of Authorizationmaxor4242No ratings yet
- Referral Letter: Employees State Insurance CorporationDocument1 pageReferral Letter: Employees State Insurance CorporationafakraipurNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceKavitha KesavanNo ratings yet
- SHIFWDocument3 pagesSHIFWmandawa786No ratings yet
- TLE Teachers F6Document6 pagesTLE Teachers F6Gerald YabutNo ratings yet
- AL Molecular Diagnostic Laboratory Inc.: Comments: Important NoticeDocument2 pagesAL Molecular Diagnostic Laboratory Inc.: Comments: Important NoticeNikka JunioNo ratings yet
- Online Advertising Online CostDocument6 pagesOnline Advertising Online CostAnam Abdul QayyumNo ratings yet
- Total Amount Without Taxes Total Amount in Words: SelectDocument3 pagesTotal Amount Without Taxes Total Amount in Words: SelectUmesh MishraNo ratings yet
- Fap Turbo GuideDocument71 pagesFap Turbo GuideUchiha AzuranNo ratings yet
- Syabas-Guideline For Water SupplyDocument2 pagesSyabas-Guideline For Water SupplyShamsul Bahrin SulaimanNo ratings yet
- Grand Strategy MatrixDocument12 pagesGrand Strategy MatrixYogita WaghNo ratings yet
- Assignment On PathaoDocument18 pagesAssignment On PathaoGendhlf TornNo ratings yet
- CHAPTER 1 - The Nature and Importance of Entrepreneurs Learning ObjectivesDocument30 pagesCHAPTER 1 - The Nature and Importance of Entrepreneurs Learning Objectiveszulfi12345No ratings yet
- HISTORYDocument2 pagesHISTORYNandini GoelNo ratings yet
- CT SS For Student Oct2018Document5 pagesCT SS For Student Oct2018Nabila RosmizaNo ratings yet
- Priti I Iiiiii 1Document93 pagesPriti I Iiiiii 1ArmanNo ratings yet
- Corporate Governance Failure at Satyam Quiz3Document2 pagesCorporate Governance Failure at Satyam Quiz3Deepak MatlaniNo ratings yet
- Journalof TourismJune 2015Document103 pagesJournalof TourismJune 2015pratolectusNo ratings yet
- King, Alexis Orcio: Kawanihan NG Rentas InternasDocument3 pagesKing, Alexis Orcio: Kawanihan NG Rentas InternasAlexis KingNo ratings yet
- InvoiceDocument1 pageInvoiceSoumyadeep DuttaNo ratings yet
- 7.) Chapter 2 (How Economic Issues Affect Business)Document7 pages7.) Chapter 2 (How Economic Issues Affect Business)John AustinNo ratings yet
- EVNAnnual Report 2018Document46 pagesEVNAnnual Report 2018Dương NguyễnNo ratings yet
- Post Qua Report FOAM ALJONDocument4 pagesPost Qua Report FOAM ALJONKim Patrick VictoriaNo ratings yet
- Material For The 28th ACSIC Conference 2015 Taiwan Taiwan SMEGDocument21 pagesMaterial For The 28th ACSIC Conference 2015 Taiwan Taiwan SMEGzulfikar husinNo ratings yet
- Tan Tek Beng v. DavidDocument4 pagesTan Tek Beng v. Davidroyel arabejoNo ratings yet
- DesignXplorer Users GuideDocument410 pagesDesignXplorer Users GuidekaranbeeshmNo ratings yet
- White Gold Opportunities For Dairy Secto PDFDocument207 pagesWhite Gold Opportunities For Dairy Secto PDFFrancis Mwangi ChegeNo ratings yet
- Henkel Ibérica PPTDocument10 pagesHenkel Ibérica PPTAmey LimayeNo ratings yet
- Exercise 3-Bar Graphs: Directions For Questions 1 To 5Document5 pagesExercise 3-Bar Graphs: Directions For Questions 1 To 5avinashNo ratings yet
- ULANGANDocument5 pagesULANGANRama Nur Anggrit PratamaNo ratings yet
- Soa SIA Bab 7 INDIVIDUDocument4 pagesSoa SIA Bab 7 INDIVIDUratnasmNo ratings yet
- Ladawna Cowings Professional Resume-2Document1 pageLadawna Cowings Professional Resume-2api-661314689No ratings yet
- Irc Kit Part F (Business Valuations)Document16 pagesIrc Kit Part F (Business Valuations)Amir ArifNo ratings yet