You might also like
- Case PresentaionDocument7 pagesCase Presentaiongulshan araNo ratings yet
- Template Duty ReportDocument6 pagesTemplate Duty ReportJefri SusantoNo ratings yet
- Yosefin Eka Pembimbing: Dr. Anik W., Sp. PK (K)Document33 pagesYosefin Eka Pembimbing: Dr. Anik W., Sp. PK (K)Yosefin EkaNo ratings yet
- Nursing Process 3Document10 pagesNursing Process 3Shubhra Sheoran100% (1)
- Surgery PortDocument5 pagesSurgery Portabenezer g/kirstosNo ratings yet
- Morning Report: Monday, 8 May 2017Document25 pagesMorning Report: Monday, 8 May 2017HarisNo ratings yet
- Hypocalcemia, Hypoparathyroid WahyuDocument27 pagesHypocalcemia, Hypoparathyroid WahyuFerdinando BaehaNo ratings yet
- Heteroanamnesa Chief Complaint: Coffe Ground Vomiting History of Present IllnessDocument6 pagesHeteroanamnesa Chief Complaint: Coffe Ground Vomiting History of Present IllnessIka AyuNo ratings yet
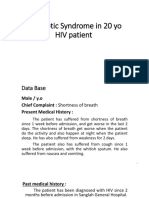
- MR Sindrom Nefrotik 1 Agustus 17Document12 pagesMR Sindrom Nefrotik 1 Agustus 17Ridho CahyaNo ratings yet
- Tajuddin Tumor ParuDocument13 pagesTajuddin Tumor ParuJuli2022 Semnol-SemsaNo ratings yet
- Incompatible Crossmatch in Patient With CKD: Hariogie Putradi Moderator: Dr. Siti Fatonah, SP - PKDocument136 pagesIncompatible Crossmatch in Patient With CKD: Hariogie Putradi Moderator: Dr. Siti Fatonah, SP - PKhariogieNo ratings yet
- Critical Care Concept Map Part 2Document10 pagesCritical Care Concept Map Part 2api-546041342No ratings yet
- Case HistoryDocument10 pagesCase HistorysharenNo ratings yet
- Morning ReportDocument27 pagesMorning ReportDody PrasetyaNo ratings yet
- Clinical Conference 21 August 2022: Eria (New Case)Document16 pagesClinical Conference 21 August 2022: Eria (New Case)mujahidah nursinNo ratings yet
- TN Ahmad KusaeriDocument5 pagesTN Ahmad KusaeriCristian RajagukgukNo ratings yet
- Case Study On Acute Gastroenteritis and Acid Peptic-2Document15 pagesCase Study On Acute Gastroenteritis and Acid Peptic-2FHAMITHANo ratings yet
- MR DOC KAD DR HeriDocument16 pagesMR DOC KAD DR HeriIffaNo ratings yet
- Case Based DiscussionDocument49 pagesCase Based DiscussionMaulana IbrahimNo ratings yet
- DK Gastro 2 - CA PankreasDocument111 pagesDK Gastro 2 - CA Pankreasdenina setyaNo ratings yet
- A. Patient'S Identity: Pale Conjunctiva +/+Document20 pagesA. Patient'S Identity: Pale Conjunctiva +/+Mutiara JihadNo ratings yet
- MR R 26 6-3 2017 MR W Fix AMS Septic AKIDocument15 pagesMR R 26 6-3 2017 MR W Fix AMS Septic AKISafira RNo ratings yet
- Case Presentation 26 NOVEMBER 2020Document57 pagesCase Presentation 26 NOVEMBER 2020Yosua Butar ButarNo ratings yet
- 1tflfhgayk5abfaqnvndrzqiDocument2 pages1tflfhgayk5abfaqnvndrzqidevendra4200.dkNo ratings yet
- DK Gastro KonsulDocument48 pagesDK Gastro Konsuldenina setyaNo ratings yet
- 325 Care Plan - 1Document17 pages325 Care Plan - 1mp1757No ratings yet
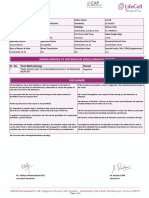
- Inborn Errors of Metabolism (Iem) Summary Report: Sr. No. Test Methodology Result Test TypeDocument2 pagesInborn Errors of Metabolism (Iem) Summary Report: Sr. No. Test Methodology Result Test TypeMallikharjunaRao medaNo ratings yet
- Template MRDocument27 pagesTemplate MRdipo buyerNo ratings yet
- Case Protocol - MucinousDocument6 pagesCase Protocol - MucinousApmc SchwartzNo ratings yet
- IM AdconDocument28 pagesIM AdconCla SantosNo ratings yet
- DK IKA 1 - Ogie RevDocument193 pagesDK IKA 1 - Ogie RevhariogieNo ratings yet
- Nursing Care Plan: Ha Noi Medical UniversityDocument17 pagesNursing Care Plan: Ha Noi Medical UniversityThảo LÊNo ratings yet
- Contoh Morning ReportDocument23 pagesContoh Morning ReportDaondy Friarsa SoehartoNo ratings yet
- Kasus Stase Nefro 4Document40 pagesKasus Stase Nefro 4Karina NilasariNo ratings yet
- Complex Care Concept MapDocument12 pagesComplex Care Concept Mapapi-508434862No ratings yet
- RAD RLE MCN 6 Case StudyDocument9 pagesRAD RLE MCN 6 Case StudyCathleen Nasis Forrosuelo100% (2)
- Friday 2-2-2018 Multiple MyelomaDocument20 pagesFriday 2-2-2018 Multiple MyelomaJefri SusantoNo ratings yet
- Its Just HoaxDocument10 pagesIts Just HoaxArkhan HanafiNo ratings yet
- Patient Data BaseDocument5 pagesPatient Data Basequina mjNo ratings yet
- MR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHDocument24 pagesMR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHIka AyuNo ratings yet
- Patient DemographicsDocument9 pagesPatient DemographicsIzaan Ahmed KhanNo ratings yet
- DK IPD 3 - Ogie AsitesDocument174 pagesDK IPD 3 - Ogie AsiteshariogieNo ratings yet
- Case Presentation: by Femi Liz Sanjana AugusthyDocument31 pagesCase Presentation: by Femi Liz Sanjana AugusthyBlessyNo ratings yet
- Abdul AzizDocument5 pagesAbdul AzizFakhrur RoziNo ratings yet
- Clinical 2Document21 pagesClinical 2api-487423840No ratings yet
- Concept MapDocument15 pagesConcept Mapapi-495456666No ratings yet
- Case Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172Document18 pagesCase Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172AmalinNo ratings yet
- DK Gastro KonsulDocument56 pagesDK Gastro Konsuldenina setyaNo ratings yet
- Case Protocol - Breast MucinousDocument6 pagesCase Protocol - Breast MucinousApmc SchwartzNo ratings yet
- Case Study of Patient With CholelithiasisDocument3 pagesCase Study of Patient With CholelithiasisBer AnneNo ratings yet
- Complex Care Plan 1Document12 pagesComplex Care Plan 1api-496883420No ratings yet
- Case Presentation - Visceral LeishmaniaDocument18 pagesCase Presentation - Visceral LeishmaniaAAANo ratings yet
- FINAL CervicalCA7BDocument6 pagesFINAL CervicalCA7BRommel OliverasNo ratings yet
- Rational Laboratory and Diagnostic TestsDocument26 pagesRational Laboratory and Diagnostic TestsCeline dela cruzNo ratings yet
- Duty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeDocument6 pagesDuty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeCristian RajagukgukNo ratings yet
- MR AckdDocument16 pagesMR AckdHananya ManroeNo ratings yet
- Morning Report: Dr. Dikara WS Maulidy, SP - PDDocument24 pagesMorning Report: Dr. Dikara WS Maulidy, SP - PDBethari Abi SafitriNo ratings yet
- DK Endokrin Mola OgieDocument51 pagesDK Endokrin Mola OgiehariogieNo ratings yet
- MR - Suardi Tumor Paru + Efusi Pleura KiriDocument14 pagesMR - Suardi Tumor Paru + Efusi Pleura KiritiarapolarisiriuzNo ratings yet
- OpenTexas Checklist Overnight Youth Camp: FamiliesDocument3 pagesOpenTexas Checklist Overnight Youth Camp: FamiliesRebecca Salinas100% (1)
- 8 (1965) Adotado em 1966Document510 pages8 (1965) Adotado em 1966Brune C. BonassiNo ratings yet
- Clinical Diagnostic Criteria For Dementia AssociatDocument20 pagesClinical Diagnostic Criteria For Dementia AssociatAnderson Cassol DozzaNo ratings yet
- AARC Clinical Practice Guideline - Management of Airway EmergenciesDocument7 pagesAARC Clinical Practice Guideline - Management of Airway EmergenciesdoterofthemosthighNo ratings yet
- Juvenile Idiopathic Arthritis (Jia) : IAP UG Teaching Slides 2015-16Document15 pagesJuvenile Idiopathic Arthritis (Jia) : IAP UG Teaching Slides 2015-16KathirNo ratings yet
- K.R. Holcomb/Medical Veritas 6 (2009) 1925-1936Document12 pagesK.R. Holcomb/Medical Veritas 6 (2009) 1925-1936omega1966No ratings yet
- Hemodialisis Sustained Low-Efficiency Dialysis: Indikasi Dan PenerapannyaDocument7 pagesHemodialisis Sustained Low-Efficiency Dialysis: Indikasi Dan Penerapannyaatun hayatunNo ratings yet
- Nurse'Sdrug Handbook Jones & Bartlett Learning 14 Edition 2015Document2 pagesNurse'Sdrug Handbook Jones & Bartlett Learning 14 Edition 2015Bianca Nicole Gacad FernandezNo ratings yet
- ECG Workshop STUDENTDocument9 pagesECG Workshop STUDENToyim sNo ratings yet
- Hannover Polytrauma Score.4Document2 pagesHannover Polytrauma Score.4Azmi FarhadiNo ratings yet
- Acute AppendicitisDocument36 pagesAcute AppendicitisOlivia CristieNo ratings yet
- Empyema Thoracis: Clinical Medicine Insights: Circulatory, Respiratory and Pulmonary MedicineDocument8 pagesEmpyema Thoracis: Clinical Medicine Insights: Circulatory, Respiratory and Pulmonary MedicinerinayondaNo ratings yet
- LF0125A - Package Insert - Comfilcon A - Biofinity - Sphere Toric MultifocalDocument5 pagesLF0125A - Package Insert - Comfilcon A - Biofinity - Sphere Toric MultifocalSanela BajramovicNo ratings yet
- Implementation of New Safety Protocols of Calle Arco Restaurant in Pagsanjan, Laguna During Pandemic CrisisDocument42 pagesImplementation of New Safety Protocols of Calle Arco Restaurant in Pagsanjan, Laguna During Pandemic CrisisOliveros John Brian R.No ratings yet
- Acute Generalized Exanthematous Pustulosis: Sima HalevyDocument18 pagesAcute Generalized Exanthematous Pustulosis: Sima HalevyDody PrasetyaNo ratings yet
- Hypersensitivity Reactions (Immunologic Tissue Injury)Document17 pagesHypersensitivity Reactions (Immunologic Tissue Injury)Revathi NerusuNo ratings yet
- Limb Lengthening Surgery by Ilizarov Methodology PDFDocument3 pagesLimb Lengthening Surgery by Ilizarov Methodology PDFJessica Saing100% (1)
- Glycogen Storage Diseases of Muscle Chapter 39 PDFDocument26 pagesGlycogen Storage Diseases of Muscle Chapter 39 PDFIsaac Mackliz VillegasNo ratings yet
- Trichuris Trichiura: Lecture By: Maha Gamal AldeinDocument20 pagesTrichuris Trichiura: Lecture By: Maha Gamal AldeinMohammad DweibNo ratings yet
- Pharmacy Daily 2nd Nov 2023Document5 pagesPharmacy Daily 2nd Nov 2023Marinero CzarNo ratings yet
- Factors Impacting Food Workers and Managers Safe Food Preparation PracticesDocument28 pagesFactors Impacting Food Workers and Managers Safe Food Preparation PracticesSteffi Grace100% (1)
- Principles of Inheritance and VariationsDocument65 pagesPrinciples of Inheritance and VariationsArmanNo ratings yet
- Medical and Surgical Nursing - IIDocument2 pagesMedical and Surgical Nursing - IIYAMINIPRIYANNo ratings yet
- Group 3 Reporting OutlineDocument6 pagesGroup 3 Reporting Outline「 」No ratings yet
- A.offer D. Furniture: HumanDocument5 pagesA.offer D. Furniture: Humansoyeondan bangtanNo ratings yet
- The Language of AnatomyDocument7 pagesThe Language of AnatomyLinziJaeOnelNo ratings yet
- Chapter I 5Document51 pagesChapter I 5RamNo ratings yet
- Nascop Indicators ManualDocument85 pagesNascop Indicators Manualjwedter1No ratings yet
- Section 8. Renal Problems: 1. A. B. C. D. Ans: B PTS: 1 2. A. B. C. D. Ans: B PTS: 1 3Document8 pagesSection 8. Renal Problems: 1. A. B. C. D. Ans: B PTS: 1 2. A. B. C. D. Ans: B PTS: 1 3AliNo ratings yet
- Artikel 1Document11 pagesArtikel 1wardatul UllyaNo ratings yet