You might also like
- Team-Based Oncology Care: The Pivotal Role of Oncology NavigationFrom EverandTeam-Based Oncology Care: The Pivotal Role of Oncology NavigationLillie D. ShockneyNo ratings yet
- Role of Nursing Staff in Patient Centric Care, Patient Safety and Hospital Infection ControlDocument31 pagesRole of Nursing Staff in Patient Centric Care, Patient Safety and Hospital Infection ControlVincy MacwanNo ratings yet
- Patient Safty Goals ......Document59 pagesPatient Safty Goals ......MemeNo ratings yet
- CM3, CU14, - PA, CanvasDocument16 pagesCM3, CU14, - PA, CanvasMichelle Gliselle Guinto MallareNo ratings yet
- Ignatavicius: Medical-Surgical Nursing, 6 EditionDocument3 pagesIgnatavicius: Medical-Surgical Nursing, 6 EditionTam HenmanNo ratings yet
- Dr. Mohamed Mosaad Hasan MD, MPH, CPHQ, CPPS, GbssDocument48 pagesDr. Mohamed Mosaad Hasan MD, MPH, CPHQ, CPPS, GbssKristine Marie PateñoNo ratings yet
- Medical Ethics BNTDocument12 pagesMedical Ethics BNTSahil FayazNo ratings yet
- Patient Safety: The Challenges of Health-Providers and Policy-MakersDocument25 pagesPatient Safety: The Challenges of Health-Providers and Policy-Makersvalerie violaNo ratings yet
- Unit 5-7Document38 pagesUnit 5-7Lovelights ZamoraNo ratings yet
- Lecture 5Document45 pagesLecture 5marwajr2509No ratings yet
- 6 Understanding and Managing Clinical RiskDocument4 pages6 Understanding and Managing Clinical Riskanojan100% (1)
- Total Quality Management - Nursing ManagementDocument6 pagesTotal Quality Management - Nursing ManagementFatima Hyghia HimponNo ratings yet
- Patient Care PDFDocument310 pagesPatient Care PDFCindy BonghanoyNo ratings yet
- Midterm Module 2Document7 pagesMidterm Module 2DianneNo ratings yet
- Sefety and InjuryDocument24 pagesSefety and Injuryswing.sujuNo ratings yet
- Unit 4 TQMDocument20 pagesUnit 4 TQMHarini DubeyNo ratings yet
- 13 Profesionalism and Managerial SkillDocument16 pages13 Profesionalism and Managerial SkillTiaRa JuraidNo ratings yet
- 10 Patient Safety and Invasive ProceduresDocument4 pages10 Patient Safety and Invasive Proceduresanojan100% (1)
- Hospital Disclosure PolicyDocument10 pagesHospital Disclosure Policyvks7876No ratings yet
- Good Governance Practices in A HospitalDocument25 pagesGood Governance Practices in A HospitalSiddhesh KhadeNo ratings yet
- Ipsg (International Patient Safety Goals) NehaDocument19 pagesIpsg (International Patient Safety Goals) Nehanehah3943No ratings yet
- PNDSDocument9 pagesPNDSivy_espesoNo ratings yet
- Group 21 Power PointDocument19 pagesGroup 21 Power PointOyetomi AdunolaNo ratings yet
- Prinsip Profesionalisme Praktek Kedokteran Dalam Perspektif Kode EtikDocument42 pagesPrinsip Profesionalisme Praktek Kedokteran Dalam Perspektif Kode EtikDeddy Supriyadi0% (1)
- Job Description Theatre NurseDocument4 pagesJob Description Theatre NursekalumbamwakaNo ratings yet
- Introduction To Patient SafetyDocument54 pagesIntroduction To Patient Safetyrejoicedear2020No ratings yet
- Perioperative NursingDocument103 pagesPerioperative NursingRochelle Anne SorioNo ratings yet
- Why Patient Safety Is Relevant To Surgery and Invasive ProceduresDocument13 pagesWhy Patient Safety Is Relevant To Surgery and Invasive ProceduresNasriah DamayanthieNo ratings yet
- Ethics in Medical PracticeDocument35 pagesEthics in Medical PracticeMohammed AadeelNo ratings yet
- JamssurgicalconscienceDocument11 pagesJamssurgicalconsciencemahadabrata21No ratings yet
- To Err Is Human: DR Inas Alassar CPHQDocument96 pagesTo Err Is Human: DR Inas Alassar CPHQYahya HashmiNo ratings yet
- Nursing Specialties Entre in Nursing//midtermDocument4 pagesNursing Specialties Entre in Nursing//midtermfatty jaiNo ratings yet
- Clinical Reasoning ImportantDocument3 pagesClinical Reasoning ImportantKrizhel Mirja CawasNo ratings yet
- NQB Hum Fact ConcordDocument22 pagesNQB Hum Fact ConcordSophia RoseNo ratings yet
- Role of ResearchDocument5 pagesRole of ResearchAiman SiddiquiNo ratings yet
- NursingDocument23 pagesNursingRoberto EsmeleNo ratings yet
- Ethical Dilemmas.Document12 pagesEthical Dilemmas.Jennifer DixonNo ratings yet
- Course01 - Handout - What Is Patient SafetyDocument4 pagesCourse01 - Handout - What Is Patient SafetySalsa Nabila Rianti PutriNo ratings yet
- Guide - 2015 - Core Competencies For Entry-Level Practice in Acute Care Physical TherapyDocument16 pagesGuide - 2015 - Core Competencies For Entry-Level Practice in Acute Care Physical TherapySM199021No ratings yet
- Code of Ethical ConductDocument19 pagesCode of Ethical ConductNeha VermaNo ratings yet
- Ipsg # 2017 PDFDocument30 pagesIpsg # 2017 PDFDARRYLARANHA100% (1)
- Quality Standards For Health Care Organization Patients RightsDocument6 pagesQuality Standards For Health Care Organization Patients RightsLey EnhaimaNo ratings yet
- 319-4327842CF - NUR1097 Job Description & Person SpecificationDocument7 pages319-4327842CF - NUR1097 Job Description & Person SpecificationThiliniNo ratings yet
- Journal Reading: What Is The Perioperative Nurses Main Challenge When Caring For The Surgical Patient?Document5 pagesJournal Reading: What Is The Perioperative Nurses Main Challenge When Caring For The Surgical Patient?Karl KiwisNo ratings yet
- Nurse As A Knowledge WorkerDocument10 pagesNurse As A Knowledge WorkerPolycarp GekongeNo ratings yet
- Medical Office ProceduresDocument5 pagesMedical Office ProceduresJerome PardilloNo ratings yet
- THPDocument25 pagesTHPThomas KearneyNo ratings yet
- Medical Professionalism and EthicsDocument27 pagesMedical Professionalism and Ethicsatharva sawantNo ratings yet
- Clinical GovernanceDocument9 pagesClinical GovernanceSajid Rahman100% (1)
- Technological Competency As Caring: A Model For NursingDocument37 pagesTechnological Competency As Caring: A Model For Nursingalmira garciaNo ratings yet
- Ethical Practice by AbrarDocument8 pagesEthical Practice by AbrarZain HadiNo ratings yet
- Patient Safety and Clinical RiskDocument5 pagesPatient Safety and Clinical Riskshylajathomas33No ratings yet
- Clinical GovernanceDocument4 pagesClinical GovernanceGayani UdayangaNo ratings yet
- Health Care Ethics - Ncm108Document8 pagesHealth Care Ethics - Ncm108AlyNo ratings yet
- Key Points: Chapter 1: Nursing Practice TodayDocument3 pagesKey Points: Chapter 1: Nursing Practice TodaylaniNo ratings yet
- 3 Patient SafetyDocument57 pages3 Patient SafetyKNOWLEDGE FeedNo ratings yet
- Bulid Capacity To Promot HealthDocument29 pagesBulid Capacity To Promot HealthTeslim TenuNo ratings yet
- Crtical CareDocument44 pagesCrtical CarehemaanandhyNo ratings yet
- Initial Data Base FormatDocument7 pagesInitial Data Base FormatrhamhonaNo ratings yet
- Varisco Solid Pumping SolutionsDocument12 pagesVarisco Solid Pumping SolutionsCatalin FrincuNo ratings yet
- The Thermodynamic Principles of Isochoric Cryopreservation.Document18 pagesThe Thermodynamic Principles of Isochoric Cryopreservation.Boris RubinskyNo ratings yet
- Account Transfer Form: Fax Cover SheetDocument6 pagesAccount Transfer Form: Fax Cover SheetJitendra SharmaNo ratings yet
- Mercaptans Removal From Gases by Absorption Into Amines and CausticDocument8 pagesMercaptans Removal From Gases by Absorption Into Amines and Causticgopal100% (1)
- Explain Why Seed Vigor Determination Is ImportantDocument5 pagesExplain Why Seed Vigor Determination Is ImportantSolomon MbeweNo ratings yet
- MAPEH Assignment For Mr. Felicilda (Only)Document6 pagesMAPEH Assignment For Mr. Felicilda (Only)Jericho Green Gerona100% (1)
- New Approaches To Cryopreservation of Cells, Tissues, and OrgansDocument19 pagesNew Approaches To Cryopreservation of Cells, Tissues, and OrgansLaura CursaruNo ratings yet
- Professional DevelopmentDocument1 pageProfessional Developmentapi-488745276No ratings yet
- Nexgard For Dogs and Puppies Free 2 Day ShippingDocument1 pageNexgard For Dogs and Puppies Free 2 Day Shippinglyly23748No ratings yet
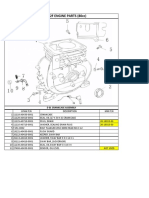
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- Spoilage of Frozen Chicken Nuggets by Toxigenic Psycrophilic FungiDocument16 pagesSpoilage of Frozen Chicken Nuggets by Toxigenic Psycrophilic FungiNIDHI BARINo ratings yet
- Boq Floor Tiling WorksDocument1 pageBoq Floor Tiling WorksISAAC KIPSEREM0% (2)
- 1-A Colored Substance That Is Spread Over A Surface and Dries To Leave A Thin Decorative or Protective Coating. Decorative or Protective CoatingDocument60 pages1-A Colored Substance That Is Spread Over A Surface and Dries To Leave A Thin Decorative or Protective Coating. Decorative or Protective Coatingjoselito lacuarinNo ratings yet
- Grade 12 - Biology Resource BookDocument245 pagesGrade 12 - Biology Resource BookMali100% (6)
- v4n3 PDFDocument168 pagesv4n3 PDFJorge RodriguezNo ratings yet
- Directory of Acredited Medical Testing LaboratoriesDocument93 pagesDirectory of Acredited Medical Testing LaboratoriesCALIDAD METROMEDICA E.UNo ratings yet
- 2019 PSRANM Conference Program FinalDocument24 pages2019 PSRANM Conference Program FinalKimmie JordanNo ratings yet
- SD502 (V22) 05.2021Document4 pagesSD502 (V22) 05.2021Beaulah HunidzariraNo ratings yet
- Nutrition AssessmentDocument7 pagesNutrition AssessmentJoyce VitalNo ratings yet
- Problem 21-02 Wright Company Spreadsheet For The Statement of Cash Flows Dec. 31 Changes Dec. 31 2020 Debits Credits 2021 Balance SheetDocument17 pagesProblem 21-02 Wright Company Spreadsheet For The Statement of Cash Flows Dec. 31 Changes Dec. 31 2020 Debits Credits 2021 Balance SheetVishal P RaoNo ratings yet
- Mini Dental ImplantsDocument11 pagesMini Dental ImplantsDario PuljićNo ratings yet
- RPLB NewDocument22 pagesRPLB NewMeta learnNo ratings yet
- First Communion: You Are The VoiceDocument10 pagesFirst Communion: You Are The VoiceErnesto Albeus Villarete Jr.No ratings yet
- Imaging-Guided Chest Biopsies: Techniques and Clinical ResultsDocument10 pagesImaging-Guided Chest Biopsies: Techniques and Clinical Resultsweni kartika nugrohoNo ratings yet
- Quality Control Argex 0032/32.50.15.08 4/10 MM EN 13055: EN 15732 NL BSB K73820/01 (1/01/2004)Document1 pageQuality Control Argex 0032/32.50.15.08 4/10 MM EN 13055: EN 15732 NL BSB K73820/01 (1/01/2004)joe briffaNo ratings yet
- Structure of AtomDocument90 pagesStructure of Atomnazaatul aaklimaNo ratings yet
- Octavia Tour BrochureDocument9 pagesOctavia Tour BrochureOvidiuIONo ratings yet
- FM 200Document3 pagesFM 200raviNo ratings yet
- Aerobic ActivitiesExercises PDFDocument14 pagesAerobic ActivitiesExercises PDFPalma, Arrabela M.No ratings yet