91% found this document useful (11 votes)
102K views2 pagesEmployee Leave Format
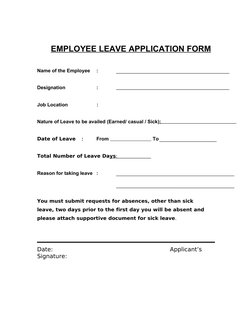
EMPLOYEE leave APPLICATION FORM Name of the Employee Designation Job Location. Nature of Leave to be availed (Earned / casual / Sick): Date of Leave : From To Total Number of Leave Days: Reason for taking leave. You must submit requests for absences, other than sick leave, two days prior to the first day you will be absent. Please attach supportive document for sick leave.
Uploaded by
Anthony NjengiCopyright
© Attribution Non-Commercial (BY-NC)
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd
91% found this document useful (11 votes)
102K views2 pagesEmployee Leave Format
EMPLOYEE leave APPLICATION FORM Name of the Employee Designation Job Location. Nature of Leave to be availed (Earned / casual / Sick): Date of Leave : From To Total Number of Leave Days: Reason for taking leave. You must submit requests for absences, other than sick leave, two days prior to the first day you will be absent. Please attach supportive document for sick leave.
Uploaded by
Anthony NjengiCopyright
© Attribution Non-Commercial (BY-NC)
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOC, PDF, TXT or read online on Scribd
- Employee Leave Application Form: Provides a form template for employees to fill when applying for leave, covering essential details like name, designation, and type of leave.
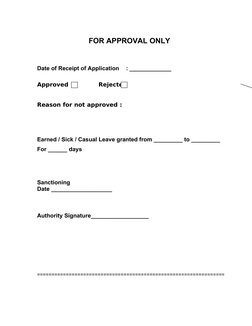
- Approval Process: Describes the formal process for approving or rejecting a leave application, including reasons for decisions and approval signatures.