You might also like
- Taking Medicines in Pregnancy: What’s Safe and What’s Not - What The Experts SayFrom EverandTaking Medicines in Pregnancy: What’s Safe and What’s Not - What The Experts SayNo ratings yet
- Some Issues To Consider While Prescribing Medications For : Pregnant and Lactating PatientsDocument25 pagesSome Issues To Consider While Prescribing Medications For : Pregnant and Lactating PatientsKishor Bajgain100% (1)
- Over-the-Counter Medications in PregnancyDocument8 pagesOver-the-Counter Medications in PregnancyAlloiBialbaNo ratings yet
- 4 - Drugs Used in Pregnancy and LactationDocument26 pages4 - Drugs Used in Pregnancy and Lactationtf.almutairi88No ratings yet
- Medications in Pregnancy 2Document16 pagesMedications in Pregnancy 2Franklin GarzaNo ratings yet
- Teratogen Information Service For Pharmacists: A Pilot StudyDocument13 pagesTeratogen Information Service For Pharmacists: A Pilot StudyfooleiNo ratings yet
- Drugs in Pregnancy and LactationDocument6 pagesDrugs in Pregnancy and LactationRidwan FajiriNo ratings yet
- Unit: 6 Pharmacology For Midwives: Prepared By: Anita Khadka M.SC Nursing 4 BatchDocument244 pagesUnit: 6 Pharmacology For Midwives: Prepared By: Anita Khadka M.SC Nursing 4 BatchAnita KhadkaNo ratings yet
- Risco Potencial Do Uso de Medicamentos Durante A Gravidez e A LactaçãoDocument6 pagesRisco Potencial Do Uso de Medicamentos Durante A Gravidez e A LactaçãoAnna Elisa Borges BarcelosNo ratings yet
- 6811-Article Text-24511-1-10-20110110Document3 pages6811-Article Text-24511-1-10-20110110Mohammed shamiul ShahidNo ratings yet
- Drug Teratogens PDFDocument26 pagesDrug Teratogens PDFgibreilNo ratings yet
- Drugs in PregnancyDocument2 pagesDrugs in PregnancyDeepankar SrigyanNo ratings yet
- Assesment of Knowledge of Analgesic Drugs in Pregnant WomenDocument6 pagesAssesment of Knowledge of Analgesic Drugs in Pregnant WomenMahrukh AmeerNo ratings yet
- Drug Use in Pregnancy & Lactation: Department of Pharmaceutical CareDocument39 pagesDrug Use in Pregnancy & Lactation: Department of Pharmaceutical CareretnodwiNo ratings yet
- PIIS0016508506008651Document29 pagesPIIS0016508506008651Ongoongoseven b. e. bNo ratings yet
- Use of Psychotropics in PregnancyDocument24 pagesUse of Psychotropics in Pregnancymanahil waqasNo ratings yet
- 4-Drugs in Obs & GyneDocument52 pages4-Drugs in Obs & Gyneapi-37033520% (2)
- Kategori Obat KehamilanDocument38 pagesKategori Obat Kehamilantheresa shintauliNo ratings yet
- Jurnal KehamilanDocument13 pagesJurnal KehamilanNuraini Putri UtamiNo ratings yet
- American Academy of Pediatrics: ABBREVIATION. FDA, Food and Drug AdministrationDocument8 pagesAmerican Academy of Pediatrics: ABBREVIATION. FDA, Food and Drug AdministrationFadjar PoernomoNo ratings yet
- Teratology & Drugs: BY DR C Sunithya Asst Prof Obs and GynaeDocument70 pagesTeratology & Drugs: BY DR C Sunithya Asst Prof Obs and GynaeMs BadooNo ratings yet
- Dr. Vikas S. Sharma MD PharmacologyDocument67 pagesDr. Vikas S. Sharma MD Pharmacologyrevathidadam55555No ratings yet
- Dr. Vikas S. Sharma MD PharmacologyDocument67 pagesDr. Vikas S. Sharma MD Pharmacologyrevathidadam55555No ratings yet
- Sato 2012Document6 pagesSato 2012triNo ratings yet
- Lijekovi U TrudnoćiDocument5 pagesLijekovi U TrudnoćiEsad MedarNo ratings yet
- J 1744-4667 2012 00096 x@10 1002 - (ISSN) 1744-4667 (CAT) Subspecialities (VI) PerinatalMedicine2015 PDFDocument6 pagesJ 1744-4667 2012 00096 x@10 1002 - (ISSN) 1744-4667 (CAT) Subspecialities (VI) PerinatalMedicine2015 PDFDrAnisha PatelNo ratings yet
- Clinical Pharmacy and Therapeutics by Cate Whittlesea and Karen HodsonDocument15 pagesClinical Pharmacy and Therapeutics by Cate Whittlesea and Karen Hodsonstella.gillesania.chenNo ratings yet
- Teratogenic Effect of Different Drugs at Different Stages in PregnancyDocument4 pagesTeratogenic Effect of Different Drugs at Different Stages in PregnancyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Drug in PregnancyDocument3 pagesDrug in PregnancyDaily DoseNo ratings yet
- 02 Pharmacotherapy in Pregnancy and LactationDocument10 pages02 Pharmacotherapy in Pregnancy and LactationAlejandra RequesensNo ratings yet
- Erythromycin Use During PregnancyDocument3 pagesErythromycin Use During Pregnancydrg Muh Rahman BurhanuddinNo ratings yet
- Drug in PregnancyDocument49 pagesDrug in PregnancyGarry B GunawanNo ratings yet
- A Review of Antihistamines Used During Pregnancy 2012 PDFDocument4 pagesA Review of Antihistamines Used During Pregnancy 2012 PDFRicardo Robles AlfaroNo ratings yet
- Prescribing in PregnancyDocument2 pagesPrescribing in Pregnancymedical studentNo ratings yet
- Amer Peds Recomm Re Psy Drugs and PregnancyDocument10 pagesAmer Peds Recomm Re Psy Drugs and Pregnancyscribd4kmhNo ratings yet
- Safe and Unsafe Drugs During PregnancyDocument12 pagesSafe and Unsafe Drugs During PregnancyfirdaustheshadowNo ratings yet
- Medication Errors & Risk ReductionDocument46 pagesMedication Errors & Risk Reductionadni_wgNo ratings yet
- Medication Safety During Pregnancy: Improving Evidence-Based PracticeDocument16 pagesMedication Safety During Pregnancy: Improving Evidence-Based PracticeANGELNo ratings yet
- TeratologyDocument34 pagesTeratologyธิติวุฒิ แสงคล้อย100% (1)
- The Nursing Process in Drug Therapy: College of Health SciencesDocument76 pagesThe Nursing Process in Drug Therapy: College of Health SciencesNat Lynne Distor TrondilloNo ratings yet
- OtcdrugDocument2 pagesOtcdrugDaffodil PearlNo ratings yet
- Pregnancy and Breast-Feeding: Mosby Items and Derived Items © 2007 by Mosby, Inc., An Affiliate of Elsevier IncDocument10 pagesPregnancy and Breast-Feeding: Mosby Items and Derived Items © 2007 by Mosby, Inc., An Affiliate of Elsevier Incsazaki224No ratings yet
- Appendix - Drug Use During PregnancyDocument6 pagesAppendix - Drug Use During PregnancySankar KuttiNo ratings yet
- The New Pregnancy and Lactation Labeling RuleDocument3 pagesThe New Pregnancy and Lactation Labeling RuleVijendra RNo ratings yet
- The Need For Safer Medication Use in Pregnancy 2013 PDFDocument4 pagesThe Need For Safer Medication Use in Pregnancy 2013 PDFRicardo Robles AlfaroNo ratings yet
- Herbal Medicine Usage Before and During Pregnancy - A Study in Northern GhanaDocument8 pagesHerbal Medicine Usage Before and During Pregnancy - A Study in Northern GhanaRaquel Orozco VargasNo ratings yet
- Sivia, 2020Document16 pagesSivia, 2020nurrahmi umamiNo ratings yet
- Do Not Copy Penalties Apply: Safety of Topical Dermatologic Medications in PregnancyDocument5 pagesDo Not Copy Penalties Apply: Safety of Topical Dermatologic Medications in Pregnancypipim septianaNo ratings yet
- Principles of Human Teratology: Drug, Chemical, and Infectious ExposureDocument7 pagesPrinciples of Human Teratology: Drug, Chemical, and Infectious ExposurenanaNo ratings yet
- Antihistamines Used During Pregnancy 2012Document4 pagesAntihistamines Used During Pregnancy 2012SRINIVASNo ratings yet
- Pregnancy Categories: Category ADocument1 pagePregnancy Categories: Category AthereseNo ratings yet
- Unit IV Drugs Used in PregnancyDocument32 pagesUnit IV Drugs Used in PregnancySuvinder singh PannuNo ratings yet
- Journal Pone 0180108Document18 pagesJournal Pone 0180108phoenixNo ratings yet
- Antibiotic GuidelinesDocument38 pagesAntibiotic GuidelinesKomang Adhi AmertajayaNo ratings yet
- Pregnancy, Breast-Feeding and Drugs Used in Dentistry: PracticeDocument14 pagesPregnancy, Breast-Feeding and Drugs Used in Dentistry: PracticeIslam FathiNo ratings yet
- Drugs Used in Pregnancy and LactationDocument13 pagesDrugs Used in Pregnancy and LactationFarina FaraziNo ratings yet
- Drugs in Pregnancy and Lactation 2021Document51 pagesDrugs in Pregnancy and Lactation 2021LU'LUIL MUNIROHNo ratings yet
- Pharma Reviewer-1Document9 pagesPharma Reviewer-1pinpindalgoNo ratings yet
- Pregnancy Breast-Feeding and Drugs Used in Dentistry JADA 2...Document14 pagesPregnancy Breast-Feeding and Drugs Used in Dentistry JADA 2...Sam YousryNo ratings yet
- Obat-Obat Dalam Masa Kehamilan Obat-Obat Dalam Masa KehamilanDocument30 pagesObat-Obat Dalam Masa Kehamilan Obat-Obat Dalam Masa KehamilanMaulana TaufikNo ratings yet
- HHFFDocument56 pagesHHFFNesru Ahmed AkkichuNo ratings yet
- Electrical Impulse Viewed: Interpretation of The ElectrocardiogramDocument41 pagesElectrical Impulse Viewed: Interpretation of The ElectrocardiogramNesru Ahmed AkkichuNo ratings yet
- 3.13 Neurologic ExaminationDocument95 pages3.13 Neurologic ExaminationNesru Ahmed AkkichuNo ratings yet
- Health Assesment ExamDocument2 pagesHealth Assesment ExamNesru Ahmed AkkichuNo ratings yet
- MOOSE (Meta-Analyses of Observational Studies in Epidemiology) ChecklistDocument2 pagesMOOSE (Meta-Analyses of Observational Studies in Epidemiology) ChecklistNesru Ahmed AkkichuNo ratings yet
- Integumentary AssessmentDocument47 pagesIntegumentary AssessmentNesru Ahmed AkkichuNo ratings yet
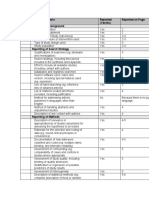
- Reporting Criteria Reported (Yes/No) Reported On Page Reporting of BackgroundDocument2 pagesReporting Criteria Reported (Yes/No) Reported On Page Reporting of BackgroundNesru Ahmed AkkichuNo ratings yet
- Concept DevelopmentDocument56 pagesConcept DevelopmentNesru Ahmed AkkichuNo ratings yet
- Mobilizing CommunityDocument1 pageMobilizing CommunityNesru Ahmed AkkichuNo ratings yet
- 10 Priya AranhaDocument6 pages10 Priya AranhaArchana SahuNo ratings yet
- Aliza Updated ResumeDocument2 pagesAliza Updated Resumeapi-359939852No ratings yet
- Intrebari Interviu Asistent MedicalDocument3 pagesIntrebari Interviu Asistent MedicalanaNo ratings yet
- Plasma Metanephrine Test: Patient Information FactsheetDocument2 pagesPlasma Metanephrine Test: Patient Information FactsheetDamigart PremiumNo ratings yet
- Effect of Human Papilloma Virus in HIV Infected Person: A Mini ReviewDocument7 pagesEffect of Human Papilloma Virus in HIV Infected Person: A Mini ReviewKIH 20162017No ratings yet
- Rhomboid Flap For Pilonidal Sinus - Our ExperienceDocument5 pagesRhomboid Flap For Pilonidal Sinus - Our ExperienceKhalidHussainNo ratings yet
- The Legal Bases of Special EducationDocument14 pagesThe Legal Bases of Special EducationMaria Dulcinea Basbas86% (7)
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)
- Art Comparison Essay ExampleDocument5 pagesArt Comparison Essay Exampleflrzcpaeg100% (2)
- Science3 Q1 W4 Proper Use HandlingDocument50 pagesScience3 Q1 W4 Proper Use HandlingGina Contalba TubeoNo ratings yet
- Why Is Research Important - NHS GroupDocument8 pagesWhy Is Research Important - NHS GroupRoxan PacsayNo ratings yet
- Circadian RhythmsDocument2 pagesCircadian RhythmsOmar Saleh100% (1)
- Eritro Papulo Skuamosa 2021Document47 pagesEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- Factories ActDocument64 pagesFactories ActKrishna Kaushik100% (1)
- The Peat WhispererDocument85 pagesThe Peat Whispererzarrin77100% (6)
- Sattvika Dite-YakubDocument6 pagesSattvika Dite-Yakubyakubjacob100% (1)
- Internal Audit Ratings GuideDocument19 pagesInternal Audit Ratings Guidesanranist2100% (3)
- I-Stat 1 Quick Reference Guide 716942-00l CompressedDocument7 pagesI-Stat 1 Quick Reference Guide 716942-00l Compressedنجلاء الطلحيNo ratings yet
- GWC - Company ProfileDocument4 pagesGWC - Company Profileelrajil100% (1)
- Position Paper TopicsDocument2 pagesPosition Paper TopicskinodecuirNo ratings yet
- Ion Breeding Policy - 2006 & 2010Document42 pagesIon Breeding Policy - 2006 & 2010Ulhas GaikwadNo ratings yet
- Microbial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Document7 pagesMicrobial Limits Tests: The Difference Between "Absence of Objectionable Microorganisms" and "Absence of Specified Microorganisms"Jai MurugeshNo ratings yet
- Presentation On PDSDocument14 pagesPresentation On PDSShiva TantiNo ratings yet
- Grade 9 Solid Waste Management Teachers - GuideDocument32 pagesGrade 9 Solid Waste Management Teachers - GuideNicole Angela NavarroNo ratings yet
- Pengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseDocument9 pagesPengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseTjatur SurantullohNo ratings yet
- Chapter 01Document22 pagesChapter 01kita5437100% (1)
- Hba1C: Quality System CertifiedDocument4 pagesHba1C: Quality System CertifiedNonameNo ratings yet
- Abnormal Illness BehaviorDocument7 pagesAbnormal Illness Behavioransha2011p0% (1)
- Flygt IOM 3152-181Document56 pagesFlygt IOM 3152-181veromesa0% (1)
- Peri Quiz Board 219Document2 pagesPeri Quiz Board 219Melody Barredo50% (2)
- Comparison of Intraocular Pressure After Water Drinking Test in Primary Open Angle Glaucoma Patients Controlled With Latanoprost and TrabeculectomyDocument7 pagesComparison of Intraocular Pressure After Water Drinking Test in Primary Open Angle Glaucoma Patients Controlled With Latanoprost and TrabeculectomyDimas Djiwa DNo ratings yet