You might also like
- Bicycle Engine Kit Installation Guide - Raw 80ccDocument9 pagesBicycle Engine Kit Installation Guide - Raw 80ccSokitome0% (1)
- C0904 091814 PDFDocument54 pagesC0904 091814 PDFBuddy JohnsonNo ratings yet
- Presentaion On Inclusiveness Chapter 3Document50 pagesPresentaion On Inclusiveness Chapter 3Addi88% (17)
- Happiness Coaching NewDocument28 pagesHappiness Coaching NewMahesh RaoNo ratings yet
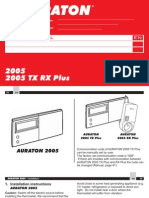
- Auraton 2005Document24 pagesAuraton 2005Muhidin KozicaNo ratings yet
- Constellation Pharma (CNST) ThesisDocument17 pagesConstellation Pharma (CNST) Thesisjulia skripka-serry100% (2)
- Chapter 08 - Ion Exchange, Water Demineralization & Resin TestingDocument23 pagesChapter 08 - Ion Exchange, Water Demineralization & Resin TestingMohamed ElbehlilNo ratings yet
- Analysis of Efficacy of Functional Appliances On Mandibular Growth PDFDocument7 pagesAnalysis of Efficacy of Functional Appliances On Mandibular Growth PDFNataly ComettaNo ratings yet
- Naufal Hafizh - Personal Statement For University of WarwickDocument2 pagesNaufal Hafizh - Personal Statement For University of WarwickNaufalNo ratings yet
- Human Factors Systems Approach To Healthcare Quality and Patient SafetyDocument12 pagesHuman Factors Systems Approach To Healthcare Quality and Patient SafetyAbhishek Shukla100% (1)
- Architecture: Passive Design With ClimateDocument39 pagesArchitecture: Passive Design With ClimateamenrareptNo ratings yet
- Medical Device Technologies: A Systems Based Overview Using Engineering StandardsFrom EverandMedical Device Technologies: A Systems Based Overview Using Engineering StandardsNo ratings yet
- ProtocoloDocument9 pagesProtocoloFamilia Chica SoteloNo ratings yet
- Class II Treatment With Functional Appliances: A Meta-Analysis of Short-Term Treatment EffectsDocument15 pagesClass II Treatment With Functional Appliances: A Meta-Analysis of Short-Term Treatment EffectsReshamIrshadNo ratings yet
- Septum Deviasi PDFDocument9 pagesSeptum Deviasi PDFErick DjuandaNo ratings yet
- PRISMA For Abstracts PDFDocument13 pagesPRISMA For Abstracts PDFVirgínia MouraNo ratings yet
- Hudson Engel-Hills Winberg 2018-With-Cover-Page-V2Document13 pagesHudson Engel-Hills Winberg 2018-With-Cover-Page-V2api-579110816No ratings yet
- Treatment Effectiveness of Frankel Function RegulaDocument13 pagesTreatment Effectiveness of Frankel Function RegulaSilvia Marcela RojasNo ratings yet
- Maxillary Molar Distalization With Noncompliance Intramaxillary Appliances in Class II MalocclusionDocument8 pagesMaxillary Molar Distalization With Noncompliance Intramaxillary Appliances in Class II MalocclusionMarcelo CostaNo ratings yet
- Angle 2007 Vol. 77, No. 2, Pp. 376-381Document6 pagesAngle 2007 Vol. 77, No. 2, Pp. 376-381André MéndezNo ratings yet
- Article Review (Sample)Document5 pagesArticle Review (Sample)Shahzad AhmadNo ratings yet
- Metanalis Efectoss Producidos Por El TwinDocument7 pagesMetanalis Efectoss Producidos Por El TwinnadiaNo ratings yet
- Short-Term Treatment Effects Produced by The Twin-Block Appliance: A Systematic Review and Meta-AnalysisDocument7 pagesShort-Term Treatment Effects Produced by The Twin-Block Appliance: A Systematic Review and Meta-AnalysisYeraldin EspañaNo ratings yet
- Short-Term Treatment Effects Produced by The Twin-Block Appliance: A Systematic Review and Meta-AnalysisDocument7 pagesShort-Term Treatment Effects Produced by The Twin-Block Appliance: A Systematic Review and Meta-AnalysisYeimi ArdilaNo ratings yet
- Learning Curve Case StudyDocument31 pagesLearning Curve Case StudyRowena CahintongNo ratings yet
- Van Midden Dorp 2013Document14 pagesVan Midden Dorp 2013Raveli KalvinNo ratings yet
- Three-Way Stopcock As Breathing Circuit in Anesthetic Procedures On Wistar Rats As Animal Models in ResearchDocument7 pagesThree-Way Stopcock As Breathing Circuit in Anesthetic Procedures On Wistar Rats As Animal Models in Researchfita triastuti /ananda syifa ahmad syamilNo ratings yet
- Part 1, Edition 2 Negida HandbookDocument59 pagesPart 1, Edition 2 Negida HandbookKareem ArafaNo ratings yet
- Intensive & Critical Care NursingDocument7 pagesIntensive & Critical Care NursingFernando PintoNo ratings yet
- Human Factors ArticleDocument8 pagesHuman Factors Articlerod_raul07No ratings yet
- Class II Functional Orthopaedic Treatment - A Systematic Review of Systematic ReviewsDocument19 pagesClass II Functional Orthopaedic Treatment - A Systematic Review of Systematic ReviewsMonica JohanaNo ratings yet
- TDF Theoretical Domain Framework How Inclusive AreDocument2 pagesTDF Theoretical Domain Framework How Inclusive ArejeancsixNo ratings yet
- Fundamental Care UCI Systematic Review 2021Document18 pagesFundamental Care UCI Systematic Review 2021marliivitorinoNo ratings yet
- Nursing and Patient Safety in The Operating Room: Journal of Advanced Nursing February 2008Document10 pagesNursing and Patient Safety in The Operating Room: Journal of Advanced Nursing February 2008Bung HerryNo ratings yet
- Funcapp PDFDocument17 pagesFuncapp PDFsathyaNo ratings yet
- Journal of Biomedical InformaticsDocument11 pagesJournal of Biomedical InformaticsSyeda Anum FatimaNo ratings yet
- Artigo Original - Fichamento N1Document6 pagesArtigo Original - Fichamento N1dranayhaneoliveiraNo ratings yet
- JCM 11 02308Document3 pagesJCM 11 02308Camila CorrêaNo ratings yet
- Evaluation and Grading Systems of Facial Paralysis For Facial RehabilitationDocument6 pagesEvaluation and Grading Systems of Facial Paralysis For Facial Rehabilitation孝仁No ratings yet
- Publishedversionofthe MScarticleDocument6 pagesPublishedversionofthe MScarticleKanchit SuwanswadNo ratings yet
- Study of Nasal Index Among Students of Tertiary MeDocument5 pagesStudy of Nasal Index Among Students of Tertiary MeBrown BoyNo ratings yet
- Treatment Effectiveness of FR Ankel Function Regulator On The Class III Malocclusion: A Systematic Review and Meta-AnalysisDocument12 pagesTreatment Effectiveness of FR Ankel Function Regulator On The Class III Malocclusion: A Systematic Review and Meta-AnalysisricardoNo ratings yet
- A Scientometric Analysis of The 100 Most Cited Articles On PallidotomyDocument11 pagesA Scientometric Analysis of The 100 Most Cited Articles On PallidotomywedawisnawaNo ratings yet
- Mojgan Shavakhi, Fatemeh Mohamadian, Hooman Zarif Najafi: ReviewsDocument6 pagesMojgan Shavakhi, Fatemeh Mohamadian, Hooman Zarif Najafi: ReviewskittyNo ratings yet
- From Concept Representations To Ontologies: A Paradigm Shift in Health Informatics?Document8 pagesFrom Concept Representations To Ontologies: A Paradigm Shift in Health Informatics?Triple-mNo ratings yet
- Preprints201904 0323 v1Document11 pagesPreprints201904 0323 v1sandeshj kumarNo ratings yet
- A Systematic Review On The Effect of Mechanical Stretch On Hypertrophic Scars After Burn InjuriesDocument9 pagesA Systematic Review On The Effect of Mechanical Stretch On Hypertrophic Scars After Burn Injuriesrizk86No ratings yet
- Intensive Care Unit Built Environments: A Comprehensive Literature Review (2005-2020)Document48 pagesIntensive Care Unit Built Environments: A Comprehensive Literature Review (2005-2020)Indhu JayavelNo ratings yet
- Biomecanica Revision LiteraturaDocument11 pagesBiomecanica Revision LiteraturaJorge Humberto Gil CardonaNo ratings yet
- Radiofrequency For The Treatment of Skin Laxity: Mith or TruthDocument15 pagesRadiofrequency For The Treatment of Skin Laxity: Mith or TruthalifardsamiraNo ratings yet
- Systematic Review of Mini-Implant Displacement Under Orthodontic LoadingDocument6 pagesSystematic Review of Mini-Implant Displacement Under Orthodontic LoadingmalifaragNo ratings yet
- A Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Kidney Transplantation Among ESRD Patients at Selected Hospitals at Mandya (Dist.)Document8 pagesA Study To Assess The Effectiveness of Structured Teaching Programme On Knowledge Regarding Kidney Transplantation Among ESRD Patients at Selected Hospitals at Mandya (Dist.)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Experience of Nurses From The Emergency Department Management: A Qualitative StudyDocument11 pagesExperience of Nurses From The Emergency Department Management: A Qualitative StudyMALIK MANASRAHNo ratings yet
- Kepatuhan MaskerDocument8 pagesKepatuhan MaskerKhairul AsriNo ratings yet
- International Journal of Scientific Research: Dental ScienceDocument3 pagesInternational Journal of Scientific Research: Dental ScienceDr Karishma MotwaniNo ratings yet
- Face-Bow Transfer in Prosthodontics: A Systematic Review of The LiteratureDocument8 pagesFace-Bow Transfer in Prosthodontics: A Systematic Review of The LiteratureMahmoud Ibrahem maanNo ratings yet
- Early Mobilisation in Mechanically Ventilated Patients: A Systematic Integrative Review of Definitions and ActivitiesDocument19 pagesEarly Mobilisation in Mechanically Ventilated Patients: A Systematic Integrative Review of Definitions and ActivitiesLina LatanzaNo ratings yet
- Dermal Fillers For Tear Trough Rejuvenation: A Systematic ReviewDocument12 pagesDermal Fillers For Tear Trough Rejuvenation: A Systematic ReviewPoramate PITAK-ARNNOPNo ratings yet
- Cybersecurity ResearchDocument2 pagesCybersecurity ResearchakshayNo ratings yet
- JCR 29 029 Hussein Dental Step 140401073705 Phpapp01Document8 pagesJCR 29 029 Hussein Dental Step 140401073705 Phpapp01Hari PriyaNo ratings yet
- JCM 11 02890Document25 pagesJCM 11 02890Poramate PITAK-ARNNOPNo ratings yet
- Systems Science and Systems Thinking in Public Health PDFDocument10 pagesSystems Science and Systems Thinking in Public Health PDFMubashir SheheryarNo ratings yet
- Environmental SustainabilityDocument5 pagesEnvironmental SustainabilityKhushi MishraNo ratings yet
- Ergonomics Workstation Assessment of Musculoskeletal Disorders in University of Port HarcourtDocument14 pagesErgonomics Workstation Assessment of Musculoskeletal Disorders in University of Port HarcourtMmesoma NwadiNo ratings yet
- Endocr 5Document11 pagesEndocr 5Bogdan GavrilNo ratings yet
- Radiological Protection in The Perspective of HealthDocument4 pagesRadiological Protection in The Perspective of Healthhizwa harunNo ratings yet
- Wearable Sensors For Clinical Applications in Epilepsy, Parkinson's Disease, and Stroke: A Mixed Methods Systematic ReviewDocument13 pagesWearable Sensors For Clinical Applications in Epilepsy, Parkinson's Disease, and Stroke: A Mixed Methods Systematic ReviewMANIMEGALAI M. ECENo ratings yet
- Orofacial PainDocument4 pagesOrofacial PainMudit GuptaNo ratings yet
- Translating Behavior Analysis - A Spectrum Rather Than A Road Map - PMCDocument21 pagesTranslating Behavior Analysis - A Spectrum Rather Than A Road Map - PMCPedro HenriqueNo ratings yet
- PERDEV12 Q1 M8 For TeacherDocument22 pagesPERDEV12 Q1 M8 For TeacherBEBERLIE GALOSNo ratings yet
- Petrochemicals Compendium PDFDocument730 pagesPetrochemicals Compendium PDFJUANNo ratings yet
- ASEAN Cosmetic Labeling Requirements DOCSDocument1 pageASEAN Cosmetic Labeling Requirements DOCSmilkymilkyNo ratings yet
- 300 SS TigDocument10 pages300 SS TigSameer KhanNo ratings yet
- Chapter - IDocument60 pagesChapter - IAnil ThakurNo ratings yet
- Police Dogs From Albania As Indicators of Exposure Risk To Toxoplasma Gondii, Neospora Caninum and Vector-Borne Pathogens of Zoonotic and Veterinary ConcernDocument13 pagesPolice Dogs From Albania As Indicators of Exposure Risk To Toxoplasma Gondii, Neospora Caninum and Vector-Borne Pathogens of Zoonotic and Veterinary Concernshshsh12346565No ratings yet
- Insect Milk: VocabularyDocument3 pagesInsect Milk: VocabularyChris Mae Vinson DalumpinesNo ratings yet
- Tyler Resume Updated 3 23 17Document1 pageTyler Resume Updated 3 23 17api-285213449No ratings yet
- Philippine Electrical CodeDocument14 pagesPhilippine Electrical CodeJohn Oyan EstilloreNo ratings yet
- in This Photograph, The Issue or Problem Depicted Is That We Became The Slaves of Science andDocument1 pagein This Photograph, The Issue or Problem Depicted Is That We Became The Slaves of Science andClarisse Angela Postre50% (2)
- Turnstile Design SheetDocument6 pagesTurnstile Design SheetArmstrongMasengaNo ratings yet
- Perilite Exposure and Hot Sitz BathDocument67 pagesPerilite Exposure and Hot Sitz Bathbanana cueNo ratings yet
- 3.conventional Signs and SymbolsDocument28 pages3.conventional Signs and SymbolsTirthankar DattaNo ratings yet
- PROYECTO DE INGLES CITRULINA FinalDocument60 pagesPROYECTO DE INGLES CITRULINA FinalBoris V ZuloetaNo ratings yet
- System 4 Med G 7831 - PG 85362Document76 pagesSystem 4 Med G 7831 - PG 85362jerimiah_manzonNo ratings yet
- SHDH2040 Lecture 5Document83 pagesSHDH2040 Lecture 5123 HahahaNo ratings yet
- Visual Inspection of Crimped ConnectionsDocument1 pageVisual Inspection of Crimped Connectionsvinay gayateNo ratings yet
- OTC-26068-MS Wettability Alteration of Heavy-Oil/Bitumen Containing Carbonates Using Solvents, High PH Solutions and Nano/Ionic LiquidsDocument18 pagesOTC-26068-MS Wettability Alteration of Heavy-Oil/Bitumen Containing Carbonates Using Solvents, High PH Solutions and Nano/Ionic Liquidsjose floresNo ratings yet
- 20mpe18 Aeor Assignment 3Document9 pages20mpe18 Aeor Assignment 3Shrinath JaniNo ratings yet
- Nitrox Tablice!Document6 pagesNitrox Tablice!Frane AsanovićNo ratings yet
- The Complete Aqueous Hydrochloric Acid Solutions Density-Concentration CalculatorDocument2 pagesThe Complete Aqueous Hydrochloric Acid Solutions Density-Concentration CalculatorEngr. Md. Tipu SultanNo ratings yet