You might also like
- 1 Burns and Grafts Dr. Gio Santos September 3 2021Document7 pages1 Burns and Grafts Dr. Gio Santos September 3 2021L4 CLERK - UY, Rhea Andrea F.No ratings yet
- 12b. Burns Injury (Russells Hall Hospital, UPDATED Mar 2012)Document11 pages12b. Burns Injury (Russells Hall Hospital, UPDATED Mar 2012)akshayNo ratings yet
- BurnsDocument4 pagesBurnsjuliusNo ratings yet
- Corneal Disease and Dystrophy Management PDFDocument53 pagesCorneal Disease and Dystrophy Management PDFScerbatiuc CristinaNo ratings yet
- Fever Measles Ear ProblemsDocument10 pagesFever Measles Ear ProblemsEBNo ratings yet
- L3-SURG-Burns (Aug3021)Document5 pagesL3-SURG-Burns (Aug3021)Marc Lyndon CafinoNo ratings yet
- 2014 Burn Patient Management - Clinical Practice GuidelinesDocument70 pages2014 Burn Patient Management - Clinical Practice Guidelinesd dNo ratings yet
- NCP AccDocument19 pagesNCP AccAthyrah KadirNo ratings yet
- LSEBN Initial Management of SEVERE BurnsDocument1 pageLSEBN Initial Management of SEVERE Burnskareem186No ratings yet
- Arizona Burncenter Guidelines PDFDocument20 pagesArizona Burncenter Guidelines PDFBuyungNo ratings yet
- Mod 7 & 8 Study GuidesDocument11 pagesMod 7 & 8 Study GuidesFerd RuizNo ratings yet
- Burns (NCM 112 - Medsurg)Document5 pagesBurns (NCM 112 - Medsurg)mblanco.dchNo ratings yet
- Burn Education Module 2.14.22Document22 pagesBurn Education Module 2.14.22Ashraf HusseinNo ratings yet
- Drug Study NicoleDocument6 pagesDrug Study NicoleFrancheska Nicole Delos SantosNo ratings yet
- Burns: by Victoria S. Brioso-AngDocument33 pagesBurns: by Victoria S. Brioso-AngAmanda OsbornNo ratings yet
- Symptom Management Guidelines: Radiation Dermatitis: Type of Radiation and EnergyDocument11 pagesSymptom Management Guidelines: Radiation Dermatitis: Type of Radiation and EnergyAdonanNo ratings yet
- Concept Map 4 AnsiiDocument1 pageConcept Map 4 Ansiiapi-523409624No ratings yet
- Burn Injury ABCDocument96 pagesBurn Injury ABCSheryl Ann Barit PedinesNo ratings yet
- Pleural Effusion Case PresentationDocument16 pagesPleural Effusion Case PresentationDhindee OmahoyNo ratings yet
- Drugn Study 2 0Document15 pagesDrugn Study 2 0Ken ChavezNo ratings yet
- 2nd Rotation Drug StudyDocument10 pages2nd Rotation Drug StudyKarolien Faye DongaNo ratings yet
- NCP Mandibular)Document5 pagesNCP Mandibular)yellarfNo ratings yet
- Bu VonnyDocument41 pagesBu VonnyZola IsmuNo ratings yet
- Cefuroxime Drug Study Rosemarie Llanillo BSN Ii eDocument3 pagesCefuroxime Drug Study Rosemarie Llanillo BSN Ii eFernandez, Florence NicoleNo ratings yet
- DrugStudy - 01 02 24Document3 pagesDrugStudy - 01 02 24Laurente, Patrizja Ysabel B. BSN-2DNo ratings yet
- Peri OpDocument9 pagesPeri OpggukNo ratings yet
- Burns: Alhad Naragude Final Year M.B.B.S (BJMC Pune) Dr. Pawan Chumbale M.S, MCH Plastic Surgery (Sassoon Hospital, Pune)Document93 pagesBurns: Alhad Naragude Final Year M.B.B.S (BJMC Pune) Dr. Pawan Chumbale M.S, MCH Plastic Surgery (Sassoon Hospital, Pune)EuniceGeraldineNo ratings yet
- Electrical Burn: Xantipphy Mae IbrahimDocument32 pagesElectrical Burn: Xantipphy Mae IbrahimMinette EmmanuelNo ratings yet
- CPG Bite StingsDocument10 pagesCPG Bite StingsMarvin M PulaoNo ratings yet
- Symptom Management Guidelines: Care of Malignant WoundsDocument7 pagesSymptom Management Guidelines: Care of Malignant WoundsPatrico Rillah Setiawan100% (1)
- BEC Conflict Primary Survey Module1 ENDocument16 pagesBEC Conflict Primary Survey Module1 ENOsamaNo ratings yet
- WHO-ICRC Basic Emergency Care CourseDocument74 pagesWHO-ICRC Basic Emergency Care CoursevverasanczNo ratings yet
- Clinical Practice Guidelines Cellulitis and AbscessDocument7 pagesClinical Practice Guidelines Cellulitis and AbscessAhmad Rafi Satrio PrayogoNo ratings yet
- 03 Perioperative NursingDocument3 pages03 Perioperative NursingAngeli IdrisNo ratings yet
- Burn CareDocument3 pagesBurn CareRafaela LennyNo ratings yet
- Referat Bedah Plastik RosDocument43 pagesReferat Bedah Plastik RosRisna AnnisaNo ratings yet
- Burn Injuries FdneDocument25 pagesBurn Injuries FdneRonit ChandNo ratings yet
- AMPUTATIONDocument6 pagesAMPUTATIONapi-3822433No ratings yet
- Bactericidal Inhibits Cell Wall Mucopeptide Synthesis: CeftriaxonDocument4 pagesBactericidal Inhibits Cell Wall Mucopeptide Synthesis: Ceftriaxonzesty-merr-l-akut-9424No ratings yet
- 2A - Pasay - Module 8 - ElaborateDocument23 pages2A - Pasay - Module 8 - ElaborateTrishaNo ratings yet
- Delantar 3bsna Parotidectomy Pleomorophic AdenomaDocument26 pagesDelantar 3bsna Parotidectomy Pleomorophic AdenomasharedNo ratings yet
- Healthcare 5.5 Session1Document3 pagesHealthcare 5.5 Session1JAY JR. APONNo ratings yet
- Protocolos Minnesota Piel ATBDocument8 pagesProtocolos Minnesota Piel ATBDaniel Alejandro CastrilloNo ratings yet
- Nursing Care PlansDocument16 pagesNursing Care PlansJobelle AcenaNo ratings yet
- LSEBN Burns Referral CriteriaDocument1 pageLSEBN Burns Referral CriteriaAna TataranuNo ratings yet
- Pneumonia AdultDocument1 pagePneumonia AdultRoi LevinzonNo ratings yet
- Consult Training 1Document9 pagesConsult Training 1Lumos MaximaNo ratings yet
- CaftriaxonedrugstudyDocument1 pageCaftriaxonedrugstudyAdrianne Khyle OngNo ratings yet
- NCP and Fdar.Document4 pagesNCP and Fdar.Ralph Laurent De DiosNo ratings yet
- ClindamycinDocument2 pagesClindamycinCrissah LacernaNo ratings yet
- Problem 2 ErwinDocument26 pagesProblem 2 ErwinZhy YouichiNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanIrish Paping TucyapaoNo ratings yet
- Surgery PDFDocument163 pagesSurgery PDFjoedeegan_100% (1)
- Skin and Soft Tissue Infections (Sstis) Clinical Guideline CellulitisDocument4 pagesSkin and Soft Tissue Infections (Sstis) Clinical Guideline Cellulitisཛཉཀབས0% (1)
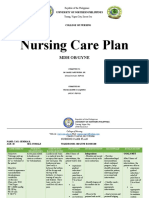
- Nursing Care Plan: MDH Ob/GyneDocument10 pagesNursing Care Plan: MDH Ob/GyneTrisha Dianne RaquenioNo ratings yet
- Approach To A Patient of Bullous DisorderDocument50 pagesApproach To A Patient of Bullous DisorderAbhirut ThakurNo ratings yet
- DRUG STUDY - DobutamineDocument3 pagesDRUG STUDY - DobutamineAjon Veloso75% (4)
- Tatalaksana Luka Bakar Pada Layanan Primer - FBBDocument31 pagesTatalaksana Luka Bakar Pada Layanan Primer - FBBfebiola sihiteNo ratings yet
- Management of Burns ReadingDocument28 pagesManagement of Burns Readinghimanshugupta811997No ratings yet
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- Differentiate Between Antimortem and Postmortem Asphyxial DeathDocument9 pagesDifferentiate Between Antimortem and Postmortem Asphyxial DeathMahnoor AyeshaNo ratings yet
- Kavitt Robert T Diagnosis and Treatment of Peptic 2019Document10 pagesKavitt Robert T Diagnosis and Treatment of Peptic 2019Nix Santos100% (1)
- Afeccion Ocular y Blefaroconjuntivitis Por Leishmania de HumanosDocument4 pagesAfeccion Ocular y Blefaroconjuntivitis Por Leishmania de HumanosPilar Sanchez GuiraoNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesJonelyn MercadoNo ratings yet
- New BookDocument2 pagesNew BookKaren Raskin KleimanNo ratings yet
- PhysioEx Exercise 7 Activity 1Document3 pagesPhysioEx Exercise 7 Activity 1CLAUDIA ELISABET BECERRA GONZALESNo ratings yet
- NURS FPX 5003 Assessment 4 Executive Summary - Community Health AssessmentDocument6 pagesNURS FPX 5003 Assessment 4 Executive Summary - Community Health AssessmentCarolyn HarkerNo ratings yet
- Pharmaceutics 3Document30 pagesPharmaceutics 3Shahid Manzoor50% (2)
- Head & Neck TumoursDocument15 pagesHead & Neck TumoursMalueth AnguiNo ratings yet
- Yang2015 Pili TortiDocument3 pagesYang2015 Pili TortiErnawati HidayatNo ratings yet
- Squash Seeds FinalDocument19 pagesSquash Seeds FinalMae TomeldenNo ratings yet
- The Safe & Effective Care EnvironmentDocument140 pagesThe Safe & Effective Care EnvironmentMoreiyamNo ratings yet
- 9.cancer of The Female Genital Tract.Document58 pages9.cancer of The Female Genital Tract.vichramNo ratings yet
- Community Based Assessment Checklist (CBAC) FormDocument3 pagesCommunity Based Assessment Checklist (CBAC) FormShubhaDavalgiNo ratings yet
- MAN 32025 Forpdf Rev0Document16 pagesMAN 32025 Forpdf Rev0alejandra ojeda anayaNo ratings yet
- 1581 PDF PDFDocument7 pages1581 PDF PDFNyinyizaw ZawNo ratings yet
- First Aid Booklet: Transition Passport / Daily Living / HealthDocument11 pagesFirst Aid Booklet: Transition Passport / Daily Living / Healthmaggie HurleyNo ratings yet
- IVT FORM 09 S 09Document1 pageIVT FORM 09 S 09lamuraoNo ratings yet
- ASHP COVID 19 Evidence TableDocument138 pagesASHP COVID 19 Evidence TableOrchid Limoso LozanoNo ratings yet
- Paraphrase DDocument62 pagesParaphrase DVignesh GNo ratings yet
- 13 - Universal Precautions: Safety Training: Eh&S - MgaDocument2 pages13 - Universal Precautions: Safety Training: Eh&S - MgaPradnya ParamitaNo ratings yet
- Hypovolemic Shock PathophysiologyDocument8 pagesHypovolemic Shock PathophysiologyKAYCEENo ratings yet
- Clinical Uses of Diode Lasers in Orthodontics PDFDocument8 pagesClinical Uses of Diode Lasers in Orthodontics PDFmonwarul azizNo ratings yet
- Curriculum For One Year Fellowship in Pain ManagementDocument8 pagesCurriculum For One Year Fellowship in Pain ManagementDr. Pankaj N SurangeNo ratings yet
- 10 Reasons Why Friendship Is ImportantDocument12 pages10 Reasons Why Friendship Is ImportantVlad CheaburuNo ratings yet
- Identification Death Dying Declaration AGE: Presented byDocument82 pagesIdentification Death Dying Declaration AGE: Presented bySaveeza Kabsha AbbasiNo ratings yet
- Ziad Abdeen PDFDocument46 pagesZiad Abdeen PDFIron Man-tcpNo ratings yet
- Internet of Nano, Bio-Nano, Biodegradable And-3-4Document2 pagesInternet of Nano, Bio-Nano, Biodegradable And-3-47d96d1b6a8No ratings yet
- CV McafeeDocument8 pagesCV Mcafeeapi-510952416No ratings yet
- Baltimore County Resource Guide December 2023Document13 pagesBaltimore County Resource Guide December 2023api-516741446No ratings yet