You might also like
- Local Flaps in Facial Reconstruction: A Defect Based ApproachFrom EverandLocal Flaps in Facial Reconstruction: A Defect Based ApproachNo ratings yet
- CPG CroupDocument4 pagesCPG CroupMarvin M PulaoNo ratings yet
- Head InjuryDocument4 pagesHead Injuryvijaykadam_ndaNo ratings yet
- Hand Pathway 4Document7 pagesHand Pathway 4api-163168129No ratings yet
- Opd, Nicu, DRDocument13 pagesOpd, Nicu, DRGiel Margareth Lindo100% (1)
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 pagesNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- 7 Abdominal TraumaDocument9 pages7 Abdominal TraumaMyrtle Yvonne RagubNo ratings yet
- BEC Conflict Primary Survey Module1 ENDocument16 pagesBEC Conflict Primary Survey Module1 ENOsamaNo ratings yet
- WHO-ICRC Basic Emergency Care CourseDocument74 pagesWHO-ICRC Basic Emergency Care CoursevverasanczNo ratings yet
- Emergency and Disaster NursingDocument9 pagesEmergency and Disaster Nursingheiyu100% (3)
- Reading Reference 1-Approach To Critically Ill Undifferntiated PatientDocument17 pagesReading Reference 1-Approach To Critically Ill Undifferntiated PatientVarshini Tamil SelvanNo ratings yet
- Delirium Screening PRISMEDocument1 pageDelirium Screening PRISMEWardah Fauziah El SofwanNo ratings yet
- Emergency Room AssessmentDocument3 pagesEmergency Room AssessmentJULIANNE BEA ACADEMIA BABIERANo ratings yet
- ED Nursing '10Document75 pagesED Nursing '10duday76No ratings yet
- Prelims Disaster Skills 1st NotesDocument6 pagesPrelims Disaster Skills 1st NotesbercoaprilgraceNo ratings yet
- A B C D E: Advanced Trauma Life Support - AtlsDocument2 pagesA B C D E: Advanced Trauma Life Support - AtlsAnnsha VeimernNo ratings yet
- Endo 5Document1 pageEndo 5Bea YmsnNo ratings yet
- Emergency and Disaster NursingDocument9 pagesEmergency and Disaster NursingDempsey AlmirañezNo ratings yet
- TLS Chapter1Document27 pagesTLS Chapter1TeojNo ratings yet
- Urological RefferalDocument12 pagesUrological Refferalmichelle octavianiNo ratings yet
- Веб-страница 2Document1 pageВеб-страница 2Zalina IvanovaNo ratings yet
- L1.1-SURG-Trauma - Burns (Aug1821)Document9 pagesL1.1-SURG-Trauma - Burns (Aug1821)Marc Lyndon CafinoNo ratings yet
- Seizures and EpilepsyDocument3 pagesSeizures and Epilepsyjoshua_villangcaNo ratings yet
- Fast DPL CTDocument6 pagesFast DPL CTnmyza89No ratings yet
- 00.00 Reference Care Plan Tonsillectomy and Adnoidectomy Post OpDocument5 pages00.00 Reference Care Plan Tonsillectomy and Adnoidectomy Post OpMarya KemmieNo ratings yet
- 00 00 Reference Care Plan Tonsillectomy and Adnoidectomy Post OpDocument5 pages00 00 Reference Care Plan Tonsillectomy and Adnoidectomy Post OpAnita LopokoiyitNo ratings yet
- Combinepdf 3Document95 pagesCombinepdf 3paruNo ratings yet
- Nursing Diagnosis Objectiv eDocument4 pagesNursing Diagnosis Objectiv eرهف الرفاعيNo ratings yet
- Toxicology and Toxinology/snake Bite: Clinical Practice GuidelinesDocument3 pagesToxicology and Toxinology/snake Bite: Clinical Practice GuidelinesEric HoNo ratings yet
- 3C3 Subgroup1 M11 PT1Document1 page3C3 Subgroup1 M11 PT1ENKELI VALDECANTOSNo ratings yet
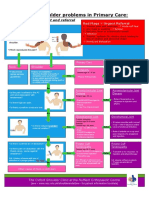
- NHS UK Diagnosis of Shoulder ProblemsDocument1 pageNHS UK Diagnosis of Shoulder ProblemsmertNo ratings yet
- Disadvantages of CT Advantages of MRI: Definitions of Neurologic FindingsDocument4 pagesDisadvantages of CT Advantages of MRI: Definitions of Neurologic FindingsAfif Al BaalbakiNo ratings yet
- Perioperative PeriodDocument14 pagesPerioperative Periodvinzy acainNo ratings yet
- Surgery PDFDocument163 pagesSurgery PDFjoedeegan_100% (1)
- Day 3Document31 pagesDay 3Sara AlramdhanNo ratings yet
- Week 1Document21 pagesWeek 1Gian Carlo BenitoNo ratings yet
- Home Care RN Skills ChecklistDocument2 pagesHome Care RN Skills ChecklistGloryJaneNo ratings yet
- ATSPDocument24 pagesATSPch wNo ratings yet
- Case Study CvaDocument33 pagesCase Study CvaArmand Bong Santiago100% (1)
- McEntee, Asst Prof Laurence Lower Back Pain A4 301120 PDFDocument2 pagesMcEntee, Asst Prof Laurence Lower Back Pain A4 301120 PDFRamesh SinghNo ratings yet
- PathopysiologyDocument14 pagesPathopysiologyAbigail Faith PretestoNo ratings yet
- Group Courage - Multiple Injured Patient (Case Discussion)Document19 pagesGroup Courage - Multiple Injured Patient (Case Discussion)Jimmy V. Venturina, Jr.No ratings yet
- 8-Suspected Stroke AlgrthmDocument1 page8-Suspected Stroke AlgrthmterminallllNo ratings yet
- NEURODISORDERSDocument24 pagesNEURODISORDERSMiden AlbanoNo ratings yet
- Deep Vein ThrombosisDocument2 pagesDeep Vein ThrombosisHimanshu PatelNo ratings yet
- Therapeutic Management of Distal Radius Fractures Slide ShowDocument38 pagesTherapeutic Management of Distal Radius Fractures Slide ShowMochammad Syarief HidayatNo ratings yet
- The Severely Ill Patient - September 2010Document11 pagesThe Severely Ill Patient - September 2010Nor Haryanti HashimNo ratings yet
- Radiation Therapy PDFDocument1 pageRadiation Therapy PDFJames Joel ReyesNo ratings yet
- Nursing Implications For Diagnostic Tests: Bone Scan and Gallium ScanDocument1 pageNursing Implications For Diagnostic Tests: Bone Scan and Gallium ScanAnisa JamitoNo ratings yet
- Truspected Stroke AlgorithmDocument4 pagesTruspected Stroke Algorithmtri wahyunoNo ratings yet
- 2A - Pasay - Module 5 - ElaborateDocument25 pages2A - Pasay - Module 5 - ElaborateTrishaNo ratings yet
- Myasthenia Gravis ReferatDocument26 pagesMyasthenia Gravis ReferatUlfa TitiswariNo ratings yet
- Anterior Uveitis: Ophthalmology Management TreeDocument2 pagesAnterior Uveitis: Ophthalmology Management TreeSandro PandurevicNo ratings yet
- General Anaesthesia in Acute Limb Ischemic Right R/ AmputationDocument20 pagesGeneral Anaesthesia in Acute Limb Ischemic Right R/ AmputationBangun Cholifa nusantaraNo ratings yet
- Nervous CompiledDocument18 pagesNervous CompiledGeraldine MaeNo ratings yet
- Marjorie ncp8Document2 pagesMarjorie ncp8Jovel CortezNo ratings yet
- Emergent Conditions (Triage and CPR)Document4 pagesEmergent Conditions (Triage and CPR)mikErlhNo ratings yet
- Corneal Disease and Dystrophy Management PDFDocument53 pagesCorneal Disease and Dystrophy Management PDFScerbatiuc CristinaNo ratings yet
- Adjustment of Secondary School Students inDocument9 pagesAdjustment of Secondary School Students inMarvin M PulaoNo ratings yet
- Nurse As Educator 6th EditionDocument20 pagesNurse As Educator 6th EditionMarvin M Pulao0% (4)
- Perfumes and Their PreparationDocument14 pagesPerfumes and Their PreparationMarvin M PulaoNo ratings yet
- Best Ref QuestionnaireDocument18 pagesBest Ref QuestionnaireMarvin M PulaoNo ratings yet
- A Study On Social Adjustment of AdolescentsDocument4 pagesA Study On Social Adjustment of AdolescentsMarvin M PulaoNo ratings yet
- Homeroom Guidance: High Five! Factors in Sound Decision-MakingDocument11 pagesHomeroom Guidance: High Five! Factors in Sound Decision-MakingMarvin M Pulao100% (2)
- Adjustment Behaviour and Its Dimensions of AdolescentDocument1 pageAdjustment Behaviour and Its Dimensions of AdolescentMarvin M PulaoNo ratings yet
- Content Validity Using A Mixed Methods Approach: Its Application and Development Through The Use of A Table of Specifications MethodologyDocument18 pagesContent Validity Using A Mixed Methods Approach: Its Application and Development Through The Use of A Table of Specifications MethodologyMarvin M PulaoNo ratings yet
- Emerging Technologies For Interactive Learning in The ICT AgeDocument22 pagesEmerging Technologies For Interactive Learning in The ICT AgeMarvin M PulaoNo ratings yet
- Instructional LeadershipDocument20 pagesInstructional LeadershipAlbert Magno CaoileNo ratings yet
- Human Resource Management and Professional DevelopmentDocument20 pagesHuman Resource Management and Professional DevelopmentRichardRaqueno80% (5)
- Three Ways of Elucidating A ConceptDocument9 pagesThree Ways of Elucidating A ConceptMarvin M Pulao100% (6)
- Structure of An Academic TextDocument9 pagesStructure of An Academic TextMarvin M PulaoNo ratings yet
- Structure of An Academic TextDocument9 pagesStructure of An Academic TextMarvin M PulaoNo ratings yet
- Most Essential Learning Competency: States Thesis Statement of An Academic TextDocument4 pagesMost Essential Learning Competency: States Thesis Statement of An Academic TextMarvin M PulaoNo ratings yet
- Beliefs and Practices During Pregnancy Labor and Delivery Postpartum and Infant Care of Women in The Second District of Ilocos Sur Philippines1Document13 pagesBeliefs and Practices During Pregnancy Labor and Delivery Postpartum and Infant Care of Women in The Second District of Ilocos Sur Philippines1Marvin M PulaoNo ratings yet
- Eimj20191102 06Document6 pagesEimj20191102 06Fred Gustavo Manrique AbrilNo ratings yet
- Oral Communication in ContextDocument191 pagesOral Communication in ContextCharlaine Gutierrez Reyes73% (11)
- Jaco Broodryk - Flexible Learning Environments - Sabbatical Report 2015Document8 pagesJaco Broodryk - Flexible Learning Environments - Sabbatical Report 2015Marvin M PulaoNo ratings yet
- Maternal and Child HealthDocument26 pagesMaternal and Child HealthMarvin M PulaoNo ratings yet
- Practical Research I: Quarter 1 - Module 2Document16 pagesPractical Research I: Quarter 1 - Module 2Marvin M Pulao75% (8)
- Coronavirus Pandemic Anxiety Scale (CPAS-11) : Development and Initial ValidationDocument9 pagesCoronavirus Pandemic Anxiety Scale (CPAS-11) : Development and Initial ValidationMarvin M PulaoNo ratings yet
- Emerging Technologies For Interactive Learning in The ICT AgeDocument22 pagesEmerging Technologies For Interactive Learning in The ICT AgeMarvin M PulaoNo ratings yet
- Booklet 1 CMDRR Training Design and ImplementationDocument56 pagesBooklet 1 CMDRR Training Design and ImplementationMarvin M Pulao100% (1)
- Gad Integrated Lesson Plan 5Document19 pagesGad Integrated Lesson Plan 5Laarni BrionesNo ratings yet
- Guide Basic Course DRR Volume 1 2014 SDC WFPDocument62 pagesGuide Basic Course DRR Volume 1 2014 SDC WFPMarvin M PulaoNo ratings yet
- Behaviour Review TheoryDocument27 pagesBehaviour Review TheoryDario Frias100% (1)
- Best Ref DRRRDocument258 pagesBest Ref DRRRMarvin M PulaoNo ratings yet
- Disaster Preparedness Training Programme: Participant Resource & Learning ModuleDocument20 pagesDisaster Preparedness Training Programme: Participant Resource & Learning ModuleMarvin M PulaoNo ratings yet
- For Drawing Themes: Qualitative Data Analysis TechniquesDocument38 pagesFor Drawing Themes: Qualitative Data Analysis TechniquesMarvin M PulaoNo ratings yet
- Case Study of Milk ProductionDocument46 pagesCase Study of Milk Productionmian21100% (2)
- BQ - Electrical Calibration Relay Bld803, NPBDocument2 pagesBQ - Electrical Calibration Relay Bld803, NPBKazuya KasumiNo ratings yet
- 7-Multiple RegressionDocument17 pages7-Multiple Regressionحاتم سلطانNo ratings yet
- A Project Report On A Study On Amul Taste of India: Vikash Degree College Sambalpur University, OdishaDocument32 pagesA Project Report On A Study On Amul Taste of India: Vikash Degree College Sambalpur University, OdishaSonu PradhanNo ratings yet
- ISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixDocument3 pagesISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixvenkatesanNo ratings yet
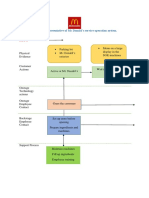
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocument2 pagesBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNo ratings yet
- Ras Shastra PPT 6Document10 pagesRas Shastra PPT 6Soham BhureNo ratings yet
- Study Notes On Isomers and Alkyl HalidesDocument3 pagesStudy Notes On Isomers and Alkyl HalidesChristian Josef AvelinoNo ratings yet
- Making Creams With Olive M 1000Document28 pagesMaking Creams With Olive M 1000Nicoleta Chiric0% (1)
- BMJ 40 13Document8 pagesBMJ 40 13Alvin JiwonoNo ratings yet
- CXC - Past - Paper - 2022 Solutions PDFDocument17 pagesCXC - Past - Paper - 2022 Solutions PDFDarren Fraser100% (1)
- Tamilnadu Shop and Establishment ActDocument6 pagesTamilnadu Shop and Establishment ActShiny VargheesNo ratings yet
- PEOPLE V JAURIGUE - Art 14 Aggravating CircumstancesDocument2 pagesPEOPLE V JAURIGUE - Art 14 Aggravating CircumstancesLady Diana TiangcoNo ratings yet
- Pengaruh Kualitas Anc Dan Riwayat Morbiditas Maternal Terhadap Morbiditas Maternal Di Kabupaten SidoarjoDocument9 pagesPengaruh Kualitas Anc Dan Riwayat Morbiditas Maternal Terhadap Morbiditas Maternal Di Kabupaten Sidoarjohikmah899No ratings yet
- Global Talent MonitorDocument30 pagesGlobal Talent Monitornitinsoni807359No ratings yet
- Biochem Nucleic Acid ReviewerDocument5 pagesBiochem Nucleic Acid ReviewerGabrielle FranciscoNo ratings yet
- Heteropolyacids FurfuralacetoneDocument12 pagesHeteropolyacids FurfuralacetonecligcodiNo ratings yet
- Ventricular Septal DefectDocument8 pagesVentricular Septal DefectWidelmark FarrelNo ratings yet
- Biopolymers: Overview of Several Properties and Consequences On Their ApplicationsDocument10 pagesBiopolymers: Overview of Several Properties and Consequences On Their ApplicationsrafacpereiraNo ratings yet
- Inducement of Rapid Analysis For Determination of Reactive Silica and Available Alumina in BauxiteDocument11 pagesInducement of Rapid Analysis For Determination of Reactive Silica and Available Alumina in BauxiteJAFAR MUHAMMADNo ratings yet
- Guideline On Smacna Through Penetration Fire StoppingDocument48 pagesGuideline On Smacna Through Penetration Fire Stoppingwguindy70No ratings yet
- CrewmgtDocument36 pagesCrewmgtDoddy HarwignyoNo ratings yet
- انظمة انذار الحريقDocument78 pagesانظمة انذار الحريقAhmed AliNo ratings yet
- Answers To Your Questions About Circumcision and HIV/AIDSDocument2 pagesAnswers To Your Questions About Circumcision and HIV/AIDSAlex BrownNo ratings yet
- Inverter 1 KW ManualDocument44 pagesInverter 1 KW ManualLeonardoNo ratings yet
- WWW Spectrosci Com Product Infracal Model CVH PrinterFriendlDocument3 pagesWWW Spectrosci Com Product Infracal Model CVH PrinterFriendlather1985No ratings yet
- Transfer and Business Taxation SyllabusDocument5 pagesTransfer and Business Taxation SyllabusamqqndeahdgeNo ratings yet
- Goals in LifeDocument4 pagesGoals in LifeNessa Layos MorilloNo ratings yet
- Basics of Fire SprinklerDocument21 pagesBasics of Fire SprinklerLeo_1982No ratings yet
- Terminologi AnatomiaDocument49 pagesTerminologi AnatomiaLuluk QurrataNo ratings yet