You might also like
- Emergent Treatment of GastroenteritisDocument28 pagesEmergent Treatment of GastroenteritisLaura Anghel-MocanuNo ratings yet
- Medscape GastritisDocument13 pagesMedscape GastritisFalaudin LaksanaNo ratings yet
- Pathophysiology of GastritisDocument2 pagesPathophysiology of GastritisFlorsean Mae Sala80% (5)
- Intra-Abdominal and Pelvic EmergenciesDocument21 pagesIntra-Abdominal and Pelvic Emergenciesqhrn48psvwNo ratings yet
- Acute Gastritis - Emedicine - 12 Jan 2011Document8 pagesAcute Gastritis - Emedicine - 12 Jan 2011Melissa KanggrianiNo ratings yet
- Diverticular Disease: Diverticulitis, Bleeding, and FistulaDocument8 pagesDiverticular Disease: Diverticulitis, Bleeding, and FistulaakashkumarpanwarNo ratings yet
- Project 101Document70 pagesProject 101Joanne Bernadette AguilarNo ratings yet
- Chapter OneDocument9 pagesChapter OneNkwenti FranklineNo ratings yet
- GastroDocument77 pagesGastroMarielle RamosNo ratings yet
- Management of Septic Peritonitis Related To Mortality in IBDDocument2 pagesManagement of Septic Peritonitis Related To Mortality in IBDRafif Abdurrahman WijisaksonoNo ratings yet
- Acute AppendicitisDocument9 pagesAcute AppendicitisSyarafina AzmanNo ratings yet
- Title - Common Bile Duct Obstruction Due To AscarisDocument3 pagesTitle - Common Bile Duct Obstruction Due To AscarisNamoc, LeninNo ratings yet
- Stomach - GastritisDocument22 pagesStomach - GastritisBîndar CristianNo ratings yet
- Background: View Media GalleryDocument6 pagesBackground: View Media Galleryprayitno tabraniNo ratings yet
- Respi, GI, GU, Repro DiseasesDocument6 pagesRespi, GI, GU, Repro DiseasesAngela OngNo ratings yet
- Questions: Peptic Ulcer DiseaseDocument11 pagesQuestions: Peptic Ulcer DiseaseNahanNo ratings yet
- Systemic Infections From GiDocument10 pagesSystemic Infections From GiJake MillerNo ratings yet
- A Case Study On Acute AppendicitisDocument56 pagesA Case Study On Acute AppendicitisIvy Mae Evangelio Vios92% (13)
- Ulkus PeptikDocument26 pagesUlkus PeptikKang MunirNo ratings yet
- Comprehensive Resume On Hepatitis ADocument9 pagesComprehensive Resume On Hepatitis AGeoffrey MasyhurNo ratings yet
- Stomach - GastritisDocument22 pagesStomach - GastritisaimanNo ratings yet
- Pediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapDocument10 pagesPediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapvgmanjunathNo ratings yet
- Dysphagia and Swallowing Disorders, MC Carty E. (2021)Document16 pagesDysphagia and Swallowing Disorders, MC Carty E. (2021)Irving Santiago SandovalNo ratings yet
- Small and Large IntestinesDocument44 pagesSmall and Large IntestinespempuladesmondsimfukwelNo ratings yet
- C Difficile DiarrheaDocument12 pagesC Difficile DiarrheaSi vis pacem...No ratings yet
- Biology Project 2018-19 Holiday HomeworkDocument7 pagesBiology Project 2018-19 Holiday HomeworkMayukhi PaulNo ratings yet
- Echinococcosis AsiyaDocument20 pagesEchinococcosis AsiyaBiswadeepan AcharyaNo ratings yet
- Neutrophils: GastritisDocument16 pagesNeutrophils: GastritisUuhhNo ratings yet
- Amoebiasis 150919181910 Lva1 App6892 PDFDocument40 pagesAmoebiasis 150919181910 Lva1 App6892 PDFMayank AhirwarNo ratings yet
- Acute Gastroenteristis Case Study GRP 3Document22 pagesAcute Gastroenteristis Case Study GRP 3juel_navarro86% (7)
- Bedah - Prekas AppendisitisDocument15 pagesBedah - Prekas AppendisitisALfianca Yudha RachmandaNo ratings yet
- G C HIV: Astrointestinal Omplications ofDocument17 pagesG C HIV: Astrointestinal Omplications ofdianaerlita97No ratings yet
- Gastroenteritis HistoryDocument8 pagesGastroenteritis HistoryLeefre Mae D NermalNo ratings yet
- GastritisDocument3 pagesGastritisShinta MasithaNo ratings yet
- PSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionDocument7 pagesPSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionMichael TobilobaNo ratings yet
- Pathology: Ascaris and After Blunt Abdominal Trauma. Children With Cystic Fibrosis Have AnDocument3 pagesPathology: Ascaris and After Blunt Abdominal Trauma. Children With Cystic Fibrosis Have AnKipyatul LizamNo ratings yet
- Peptic UlcerDocument8 pagesPeptic UlcerruhinatabassumNo ratings yet
- GastroenteritisDocument2 pagesGastroenteritisabhieghailNo ratings yet
- GastroenteritisDocument3 pagesGastroenteritisNicoleNo ratings yet
- Faciolopsiasis: History, Description Mode of Infection, Treatment & PreventionDocument4 pagesFaciolopsiasis: History, Description Mode of Infection, Treatment & PreventionSamridhi SinghNo ratings yet
- Patho AssignmentDocument17 pagesPatho AssignmentKevser UnalNo ratings yet
- Acute GastroenteritisDocument48 pagesAcute GastroenteritisAbel QuisquisNo ratings yet
- Intraabdominal InfectionsDocument17 pagesIntraabdominal InfectionsmmsNo ratings yet
- Protozoan Infections Part 2Document19 pagesProtozoan Infections Part 2Medicine SWUNo ratings yet
- Viral Gastroenteritis MCBDocument9 pagesViral Gastroenteritis MCBJake MillerNo ratings yet
- GastroenteritisDocument14 pagesGastroenteritisJils SureshNo ratings yet
- Diarrhea in Adults: EpidemiologyDocument11 pagesDiarrhea in Adults: EpidemiologyIca PalensinaNo ratings yet
- PeritonitissDocument46 pagesPeritonitissNinaNo ratings yet
- DiverticulitisDocument15 pagesDiverticulitisElisabeth MelisaNo ratings yet
- Microbiology 1Document57 pagesMicrobiology 1Kyla RamonesNo ratings yet
- Diarréia em Potros - 2007Document3 pagesDiarréia em Potros - 2007thiago.veterinariaNo ratings yet
- Recurrent Pyogenic CholangitisDocument19 pagesRecurrent Pyogenic Cholangitismayteveronica1000No ratings yet
- Skenario 2 GastroDocument31 pagesSkenario 2 GastroChendy EndriansaNo ratings yet
- El Trasplante Fecal Como Alternativa TerapeuticaDocument16 pagesEl Trasplante Fecal Como Alternativa TerapeuticaKatherine Shirley Patiño CopaNo ratings yet
- Peptic Ulcer DiseaseDocument14 pagesPeptic Ulcer DiseaseValerrie NgenoNo ratings yet
- A Me Bias IsDocument5 pagesA Me Bias IsRavinder NainawatNo ratings yet
- Diverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandDiverticulosis, A Simple Guide to the Condition, Treatment and Related DiseasesRating: 1 out of 5 stars1/5 (1)
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Epithelial CellsDocument73 pagesEpithelial CellsLouise Nicole CastroNo ratings yet
- Martial Law ReflectionDocument2 pagesMartial Law ReflectionLouise Nicole CastroNo ratings yet
- 3 1-HistoDocument7 pages3 1-HistoLouise Nicole CastroNo ratings yet
- Lecture Notes Sas 1 Sas 5Document25 pagesLecture Notes Sas 1 Sas 5Louise Nicole CastroNo ratings yet
- C. Sinensis NotesDocument6 pagesC. Sinensis NotesLouise Nicole CastroNo ratings yet
- Case 5Document27 pagesCase 5Louise Nicole CastroNo ratings yet
- Calendar of Events For National Crime Victims' Rights WeekDocument3 pagesCalendar of Events For National Crime Victims' Rights WeekIvan HerreraNo ratings yet
- Nutrition LectureDocument30 pagesNutrition LectureJovelle Sto.domingoNo ratings yet
- Guillain-Barre SyndromeDocument24 pagesGuillain-Barre SyndromeDrNorNo ratings yet
- UntitledDocument731 pagesUntitledAlvaro Delfor Umpiri MirandaNo ratings yet
- Covid PregnancyDocument3 pagesCovid PregnancyDianeNo ratings yet
- Cervicitis Symptoms, Treatment, Causes & TypesDocument1 pageCervicitis Symptoms, Treatment, Causes & Typesramit singlaNo ratings yet
- Oncology TestDocument32 pagesOncology TestPhilip Gene II MalacasNo ratings yet
- Pharma 1.13 CASE 1Document2 pagesPharma 1.13 CASE 1Aesthetics MinNo ratings yet
- Thesis Medical Surgical NursingDocument5 pagesThesis Medical Surgical Nursingafbsbwceg100% (1)
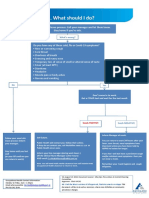
- What To Do If Youre Sick FlowchartDocument1 pageWhat To Do If Youre Sick FlowchartfuckyouNo ratings yet
- Tabes DorsalisDocument18 pagesTabes DorsalisEric ChristianNo ratings yet
- Obesity JamaDocument16 pagesObesity JamaSrinivas PingaliNo ratings yet
- What Is Physiatry 2022Document2 pagesWhat Is Physiatry 2022Victoria GonzalezNo ratings yet
- Avmed Quiz 2Document3 pagesAvmed Quiz 2Mulyantara MPNo ratings yet
- NMDAR4Document4 pagesNMDAR4Sirly PutriNo ratings yet
- Health Declaration Form D02Document1 pageHealth Declaration Form D02Hizwani ZainalNo ratings yet
- Marital RapeDocument2 pagesMarital RapeLek TupiñoNo ratings yet
- (醫學筆記) 抗生素使用 Antibiotics part.1 概論+β-lactam: by kphsien Published 97 CommentsDocument8 pages(醫學筆記) 抗生素使用 Antibiotics part.1 概論+β-lactam: by kphsien Published 97 Comments蔡宏達No ratings yet
- Nejmoa2030183 AppendixDocument34 pagesNejmoa2030183 AppendixAmna ElayanNo ratings yet
- Kendriya Vidyalaya Ins Chilka: Biology Investigatory ProjectDocument17 pagesKendriya Vidyalaya Ins Chilka: Biology Investigatory ProjectJayashree MishraNo ratings yet
- Eleanore Hatta 2023 WT HEALTH 7 UNIT 4 BackcheckDocument11 pagesEleanore Hatta 2023 WT HEALTH 7 UNIT 4 BackcheckRouel PaduaNo ratings yet
- Cerebral Concussion - PathophyDocument4 pagesCerebral Concussion - PathophyFretzgine Lou ManuelNo ratings yet
- EUROIMMUN Diagnostic Method For Hypersensitivity in Allergy Reaction FinalDocument52 pagesEUROIMMUN Diagnostic Method For Hypersensitivity in Allergy Reaction Finalgonteng sadyogaNo ratings yet
- 2023 CC Full WorkbookDocument988 pages2023 CC Full WorkbookZahra Ahmed AlzaherNo ratings yet
- Domestic Abuse: Women's AidDocument30 pagesDomestic Abuse: Women's AidiqbalNo ratings yet
- Vertigo Maneuvers Epley, Semont, Foster, and Brandt-DaroffDocument5 pagesVertigo Maneuvers Epley, Semont, Foster, and Brandt-DaroffIdoNo ratings yet
- 5-Surgical InfectionsDocument46 pages5-Surgical InfectionsAiden JosephatNo ratings yet
- 2.orthognathic Surgery - Lower JawDocument4 pages2.orthognathic Surgery - Lower JawPaul MathaiNo ratings yet
- Medicine - Irfan MasoodDocument701 pagesMedicine - Irfan MasoodAflaha KhanNo ratings yet
- DRUG STUDY (Clopidogrel)Document7 pagesDRUG STUDY (Clopidogrel)Fatima MohammedNo ratings yet