You might also like
- Neuroleptic Malignant SyndromeDocument21 pagesNeuroleptic Malignant SyndromeAndreea BujorNo ratings yet
- Adultadhdscreenertest 1Document3 pagesAdultadhdscreenertest 1FAKESIGNUPACCOUNTNo ratings yet
- Cervical Stenosis 2006Document16 pagesCervical Stenosis 2006kppsadiNo ratings yet
- Antiepileptic FullDocument60 pagesAntiepileptic FullBurning DesireNo ratings yet
- Metabolic Encephalopathies and Delirium: Panayiotis N. Varelas, MD, PHDDocument34 pagesMetabolic Encephalopathies and Delirium: Panayiotis N. Varelas, MD, PHDjorge_suoNo ratings yet
- ST John First Aid Course Questions & AnswersDocument3 pagesST John First Aid Course Questions & AnswersJames Hanlon71% (31)
- Caffeine - WikipediaDocument284 pagesCaffeine - WikipediaHisham Al-AnsariNo ratings yet
- Depression AntidepressantsDocument22 pagesDepression AntidepressantsjwsilveiraNo ratings yet
- Epilepsy & Antiepileptic Drugs: Dr. Siva Priya Sonali Thanushanthan Tivashkar Srinaath SidhantasahooDocument40 pagesEpilepsy & Antiepileptic Drugs: Dr. Siva Priya Sonali Thanushanthan Tivashkar Srinaath Sidhantasahoothanush_15No ratings yet
- PowerPoint AntidepressantsDocument29 pagesPowerPoint AntidepressantsRaeika GanjiNo ratings yet
- DMSO Potentiation Therapy (DPT) DMSO - The Magic Bullet For CancerDocument8 pagesDMSO Potentiation Therapy (DPT) DMSO - The Magic Bullet For CancerDanielaCostaNo ratings yet
- Antidepressant Side Effects 2006Document9 pagesAntidepressant Side Effects 2006Renny AnggrainiNo ratings yet
- FebuxostatDocument14 pagesFebuxostatSanjay NavaleNo ratings yet
- Antidepressant DrugsDocument55 pagesAntidepressant Drugsmaheen aurangzaib100% (2)
- Orthodontic Management in Children With Special NeedsDocument5 pagesOrthodontic Management in Children With Special NeedsAnonymous LnWIBo1GNo ratings yet
- Dermatology MCQDocument18 pagesDermatology MCQR Ratheesh100% (2)
- Uremic EncephalopathyDocument4 pagesUremic EncephalopathySandi BeyNo ratings yet
- Lung CancerDocument2 pagesLung CancerAurea Jasmine DacuycuyNo ratings yet
- Side Effects of EscitalopramDocument3 pagesSide Effects of EscitalopramIssa umulimaNo ratings yet
- Adverse Effects of ParoxetineDocument4 pagesAdverse Effects of ParoxetineIssa umulimaNo ratings yet
- Acetylcholinesterase InhibitorDocument11 pagesAcetylcholinesterase InhibitorAssassin's j :uNo ratings yet
- UntitledDocument42 pagesUntitledVivek KumarNo ratings yet
- Product Information Biltricide (Praziquantel) Name of The MedicineDocument6 pagesProduct Information Biltricide (Praziquantel) Name of The MedicinePiet Janse van RensburgNo ratings yet
- Epilepsy: Neurovascular DisordersDocument30 pagesEpilepsy: Neurovascular DisordersNdoo NdooNo ratings yet
- 22 MetabolicEncephalopathies FinalDocument19 pages22 MetabolicEncephalopathies FinalShravan BimanapalliNo ratings yet
- Side Effects of CitalopramDocument3 pagesSide Effects of CitalopramIssa umulimaNo ratings yet
- Duloxetine PDFDocument4 pagesDuloxetine PDFscribdseewalNo ratings yet
- Anti-Epilepsy Agents: DR Gareth NobleDocument50 pagesAnti-Epilepsy Agents: DR Gareth NoblekundagolNo ratings yet
- Emerging Focal Points in Depression and Anxiety: 22 ECNP Congress, IstanbulDocument92 pagesEmerging Focal Points in Depression and Anxiety: 22 ECNP Congress, Istanbuldorina.amaliaNo ratings yet
- Skeletal Muscle Relaxants and AssociatedDocument10 pagesSkeletal Muscle Relaxants and AssociatedMiguelNo ratings yet
- AnP - PsychopharmacologyDocument37 pagesAnP - PsychopharmacologyNicole JohnsonNo ratings yet
- General Principles of Pharmacology: Pharmacology Is The Study Drug Effects On Living SystemsDocument72 pagesGeneral Principles of Pharmacology: Pharmacology Is The Study Drug Effects On Living SystemsSajjul KhanNo ratings yet
- DMT of MNDDocument39 pagesDMT of MNDthelegend 2022No ratings yet
- Hospital Pharmacy Training AssignmentDocument24 pagesHospital Pharmacy Training AssignmentSathish SatzzNo ratings yet
- Drugsssss For ScrapDocument17 pagesDrugsssss For ScrapCAMILLE GAIL HADJIRANINo ratings yet
- Essential Tremor - Practice Essentials, Background, EtiologyDocument6 pagesEssential Tremor - Practice Essentials, Background, EtiologydilaNo ratings yet
- TremorDocument14 pagesTremorEcaterina LungociuNo ratings yet
- ECT PharmacologyDocument29 pagesECT PharmacologySangkaran KumarNo ratings yet
- Ejaculatory Dysfunction in Patient With Schizophrenia On SertindoleDocument4 pagesEjaculatory Dysfunction in Patient With Schizophrenia On SertindoleIda MaryaniNo ratings yet
- Amitriptyline PDFDocument3 pagesAmitriptyline PDFscribdseewalNo ratings yet
- Lec30 - Brain Protection and ResuscitationDocument30 pagesLec30 - Brain Protection and Resuscitationcitra dewiNo ratings yet
- Cerebro Lys inDocument18 pagesCerebro Lys inKathleen PalomariaNo ratings yet
- AL-Zaytoonah University of Jordan Faculty of Nursing Antipsychotic Drug Prepared By: Alaa Ali Alabbade. Alosh Al Hmrany. Ms:-Doaa MS:-HamzaDocument38 pagesAL-Zaytoonah University of Jordan Faculty of Nursing Antipsychotic Drug Prepared By: Alaa Ali Alabbade. Alosh Al Hmrany. Ms:-Doaa MS:-HamzaHamze Abdullah Al-ShawaheenNo ratings yet
- Psychiatry Drugs 2Document57 pagesPsychiatry Drugs 2Abdulmajid mohamedNo ratings yet
- Cooh Cooh NH OH: Tryptophan 5-HydroxytryptophanDocument14 pagesCooh Cooh NH OH: Tryptophan 5-HydroxytryptophankoushiksarkerNo ratings yet
- Psychological Treatment of Children and AdolescentsDocument50 pagesPsychological Treatment of Children and AdolescentsIkea BalhonNo ratings yet
- Delirium Tremens TugasDocument14 pagesDelirium Tremens TugasVeronica Yosita AnandaNo ratings yet
- Epilepsy: Rawan AlanaziDocument21 pagesEpilepsy: Rawan AlanaziMunera SultanNo ratings yet
- Epilepsy: Epilepsia (Journal) Epileptic (Graphic Novel)Document3 pagesEpilepsy: Epilepsia (Journal) Epileptic (Graphic Novel)Conie Miracle PurbaNo ratings yet
- ��تجميعات الفارما�Document4 pages��تجميعات الفارما�Turky TurkyNo ratings yet
- PI Viagra 488Document14 pagesPI Viagra 488SadulNo ratings yet
- Muscle RelaxantsDocument20 pagesMuscle RelaxantsJearanell LabraNo ratings yet
- Musculoskeletal DrugsDocument29 pagesMusculoskeletal DrugsjanulNo ratings yet
- PrognosisDocument8 pagesPrognosisallkhusairy6tuansiNo ratings yet
- Cyproheptadine - A Wonder DrugDocument5 pagesCyproheptadine - A Wonder Drugra222j239No ratings yet
- Ayurvedic Remedies For Erectile DysfunctionDocument14 pagesAyurvedic Remedies For Erectile DysfunctionAnonymous SQh10rGNo ratings yet
- Melatonina (2008) Poisoning and ToxicologyDocument3 pagesMelatonina (2008) Poisoning and ToxicologyAlumno del Doctorado FarmacologiaNo ratings yet
- Central Nervous System (CNS) Pharmacology (PCL 401) Antiepileptic/Anticonvulsants DrugsDocument33 pagesCentral Nervous System (CNS) Pharmacology (PCL 401) Antiepileptic/Anticonvulsants DrugsJoseph JohnNo ratings yet
- Source 3Document3 pagesSource 3PJHGNo ratings yet
- Drugs For Erectile DysfunctionDocument22 pagesDrugs For Erectile Dysfunctionlakshmi sravya cheenepalliNo ratings yet
- Status EpilepticusDocument42 pagesStatus EpilepticusJesse EstradaNo ratings yet
- Extrapyramidal Symptoms - StatPearls - NCBI BookshelfDocument6 pagesExtrapyramidal Symptoms - StatPearls - NCBI BookshelfFitrah RahmadhaniNo ratings yet
- Sedation or Induction Agents For Rapid Sequence Ion in AdultsDocument13 pagesSedation or Induction Agents For Rapid Sequence Ion in AdultsEllen MacDonaldNo ratings yet
- Antidepressant MedsDocument7 pagesAntidepressant Medsirish274No ratings yet
- Brain Protection and ResuscitationDocument25 pagesBrain Protection and Resuscitationcitra dewiNo ratings yet
- Frontiers in Clinical Drug Research - CNS and Neurological Disorders: Volume 9From EverandFrontiers in Clinical Drug Research - CNS and Neurological Disorders: Volume 9No ratings yet
- Society and Culture On EscitalopramDocument2 pagesSociety and Culture On EscitalopramIssa umulimaNo ratings yet
- Pharmacology of ParoxetineDocument1 pagePharmacology of ParoxetineIssa umulimaNo ratings yet
- Marketing Environment AssignmentDocument3 pagesMarketing Environment AssignmentIssa umulimaNo ratings yet
- Escitalopram Introduction and UsesDocument2 pagesEscitalopram Introduction and UsesIssa umulimaNo ratings yet
- Fluoxetine PharmacologyDocument2 pagesFluoxetine PharmacologyIssa umulimaNo ratings yet
- Binding Profile ParoxetineDocument3 pagesBinding Profile ParoxetineIssa umulimaNo ratings yet
- Administration of CitalopramDocument2 pagesAdministration of CitalopramIssa umulimaNo ratings yet
- Equality ConstraintsDocument1 pageEquality ConstraintsIssa umulimaNo ratings yet
- Quadratic ProgrammingDocument1 pageQuadratic ProgrammingIssa umulimaNo ratings yet
- HazradDocument16 pagesHazradPhan AnNo ratings yet
- Activity 4-Creative ArtsDocument3 pagesActivity 4-Creative Artsapi-568507733No ratings yet
- English AssignmentDocument7 pagesEnglish AssignmentShanzay TahirNo ratings yet
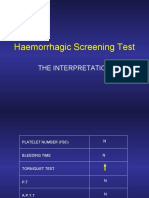
- Haemorrhagic Screening Test: The InterpretationDocument40 pagesHaemorrhagic Screening Test: The InterpretationAngel 冯晓君No ratings yet
- Sample CollectionDocument8 pagesSample CollectionwillowmaecayabyabNo ratings yet
- Pathophysiology Infective EarditisDocument3 pagesPathophysiology Infective EarditisDanielJosephLim50% (2)
- Ganoderma Ganotherapeiathefivestagesofaction - GanotherapyDocument4 pagesGanoderma Ganotherapeiathefivestagesofaction - GanotherapysakisgalanNo ratings yet
- Difference Between Bacteria and VirusDocument11 pagesDifference Between Bacteria and VirusSakib Rahman DiptoNo ratings yet
- Journal of Dental Research: Regional Anesthesia in Dental and Oral Surgery: A Plea For Its StandardizationDocument15 pagesJournal of Dental Research: Regional Anesthesia in Dental and Oral Surgery: A Plea For Its StandardizationFerdina NidyasariNo ratings yet
- FDA Inspection in India (2005 - 2012)Document11 pagesFDA Inspection in India (2005 - 2012)Asijit SenNo ratings yet
- Ductal Carcinoma in SituDocument7 pagesDuctal Carcinoma in SituLittle DevNo ratings yet
- Nursing Test Bank Introductory Mental Health Nursing 2nd Edition by Donna M WombleDocument6 pagesNursing Test Bank Introductory Mental Health Nursing 2nd Edition by Donna M WombleHarry Coston100% (35)
- Case Study Baby HDocument6 pagesCase Study Baby HSharon Williams0% (1)
- What Are AntibioticsDocument13 pagesWhat Are Antibioticsayush nayakNo ratings yet
- Basic ECG InterpretationDocument62 pagesBasic ECG Interpretationmohannadalkwiese3No ratings yet
- The Assessment and Management of Acute Pain in ChildrenDocument7 pagesThe Assessment and Management of Acute Pain in ChildrenMadyline VictoryaNo ratings yet
- Management of Ocular Chemical InjuriesDocument82 pagesManagement of Ocular Chemical InjuriesAfiqah FaizalNo ratings yet
- ANHE 426 Introduction To Animal Diseases NewDocument65 pagesANHE 426 Introduction To Animal Diseases NewSamuel MutungaNo ratings yet
- 5 Cover Letter Samples For Your Scientific ManuscriptDocument11 pages5 Cover Letter Samples For Your Scientific ManuscriptAlejandra J. Troncoso100% (2)
- Association of Early Exposure of Probiotics and Islet Autoinmmunity in The Teddy StudyDocument10 pagesAssociation of Early Exposure of Probiotics and Islet Autoinmmunity in The Teddy StudyJUAN SEBASTIAN AVELLANEDA MARTINEZNo ratings yet
- Check List Emergency Trolley: Nama Obat / Barang JLH KetDocument3 pagesCheck List Emergency Trolley: Nama Obat / Barang JLH KetablelineNo ratings yet
- Introduction To The Biology of Cancer - CourseraDocument5 pagesIntroduction To The Biology of Cancer - CourseraSamNo ratings yet
- Trimethylamine N-Oxide: The Good, The Bad and The Unknown: Health Sciences Research CommonsDocument12 pagesTrimethylamine N-Oxide: The Good, The Bad and The Unknown: Health Sciences Research CommonsVeneta GizdakovaNo ratings yet