You might also like
- DiverticulitisDocument23 pagesDiverticulitisSuhanda SaputraNo ratings yet
- IBD Ulcerative Colitis & Ghrons DiseaseDocument125 pagesIBD Ulcerative Colitis & Ghrons DiseaseDr. Ammar Khalil100% (2)
- Crohn's Disease: Natural Healing Forever, Without MedicationFrom EverandCrohn's Disease: Natural Healing Forever, Without MedicationNo ratings yet
- Uworld - SURGERYDocument55 pagesUworld - SURGERYNikxyNo ratings yet
- Stomach: Summary and Tips !Document70 pagesStomach: Summary and Tips !Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Colorectal: Another Big Topic!Document240 pagesColorectal: Another Big Topic!Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- 01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENDocument66 pages01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENMikey ZhitnitskyNo ratings yet
- 28 - IbdDocument57 pages28 - IbdsitiNo ratings yet
- Esophagus: Summary and Tips !Document75 pagesEsophagus: Summary and Tips !Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- IBD Obat Ganguan Saluran CernaDocument13 pagesIBD Obat Ganguan Saluran CernaKhumairah mohtarNo ratings yet
- Inflammatoray Bowel DiseaseDocument14 pagesInflammatoray Bowel DiseaseSadr AkrmNo ratings yet
- Ulcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryDocument71 pagesUlcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryFachry Al RafiqiNo ratings yet
- UlcerativecolitisDocument27 pagesUlcerativecolitisMohamed Abdulrazaq100% (1)
- Ulcerativecolitis 170323180448 PDFDocument88 pagesUlcerativecolitis 170323180448 PDFBasudewo Agung100% (1)
- IntussusceptionDocument14 pagesIntussusceptionAmit RamrattanNo ratings yet
- GI Fistulas: Principles and ManagementDocument27 pagesGI Fistulas: Principles and ManagementDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
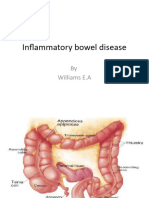
- Inflammatory Bowel DiseaseDocument52 pagesInflammatory Bowel DiseaseWilliams Emmanuel AdeyeyeNo ratings yet
- Inflammatory Bowel DiseaseDocument24 pagesInflammatory Bowel DiseaseNajla ShuaibNo ratings yet
- By Col - Abrar Hussain ZaidiDocument47 pagesBy Col - Abrar Hussain ZaidiSilvanaPutriNo ratings yet
- Inflammatory Bowel Disease (Ibd)Document28 pagesInflammatory Bowel Disease (Ibd)suhaNo ratings yet
- Inflammatory Bowel DiseaseDocument19 pagesInflammatory Bowel Diseasenathan asfahaNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CK: GastroDocument32 pagesDr. Ali's Uworld Notes For Step 2 CK: GastrouyesNo ratings yet
- Surgery: Crohn's DiseaseDocument9 pagesSurgery: Crohn's Diseaseapi-3829364No ratings yet
- Eric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafDocument18 pagesEric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafMuhammad GassanNo ratings yet
- Ministry of Education and Scientific Research) ) Al-Muthanna University College of Medicine) )Document21 pagesMinistry of Education and Scientific Research) ) Al-Muthanna University College of Medicine) )Hussein H. MahmoodNo ratings yet
- Ulcerative ColitisDocument21 pagesUlcerative ColitisShofiyyah SaniNo ratings yet
- Crohns DiseaseDocument32 pagesCrohns DiseaseMin Chi PakNo ratings yet
- 5 CD 12th EdDocument12 pages5 CD 12th Edstella.gillesania.chenNo ratings yet
- Ulcerative ColitisDocument88 pagesUlcerative ColitisYulia DjatiwardaniNo ratings yet
- Peptic Ulcer DiseaseDocument51 pagesPeptic Ulcer DiseasedocsNo ratings yet
- Inflammatory Bowel Disease .. Last EditDocument22 pagesInflammatory Bowel Disease .. Last EditRashed ShatnawiNo ratings yet
- Lecture 29 January 24th-GIDocument3 pagesLecture 29 January 24th-GIapi-26938624No ratings yet
- Intestinal Obstruction: Very Hot Surgical Topic !Document116 pagesIntestinal Obstruction: Very Hot Surgical Topic !Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Inflammatory Bowel Disease: By: Yilak G. Augst 2015Document44 pagesInflammatory Bowel Disease: By: Yilak G. Augst 2015TESFAYE YIRSAWNo ratings yet
- Curs 5Document151 pagesCurs 5Adina RomanNo ratings yet
- Inflammatory Bowel DiseaseDocument51 pagesInflammatory Bowel DiseaseTeena Chandran100% (1)
- LAPcarlberg 2016Document21 pagesLAPcarlberg 20164bm5hb2dydNo ratings yet
- GIN L9 Shabot 0708Document53 pagesGIN L9 Shabot 0708api-3799874No ratings yet
- Khalil PathoDocument43 pagesKhalil PathoMohammad zreadNo ratings yet
- Inflammatory Bowel Disease: 7 Year DR Felix MicheloDocument55 pagesInflammatory Bowel Disease: 7 Year DR Felix MicheloFreeburn SimunchembuNo ratings yet
- Valentina Miacci VI Anno 2018/2019Document20 pagesValentina Miacci VI Anno 2018/2019valentina miacciNo ratings yet
- In Brief: Cholelithiasis and CholecystitisDocument4 pagesIn Brief: Cholelithiasis and CholecystitisZazaNo ratings yet
- Breast Infections: Principles, Pathology and ManagementDocument164 pagesBreast Infections: Principles, Pathology and ManagementDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Wilm's Tumor and NeuroblastomaDocument29 pagesWilm's Tumor and NeuroblastomaDidi SudiyatmoNo ratings yet
- Inflammatory Bowel DiseaseDocument59 pagesInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiNo ratings yet
- Cholecystitis FinalDocument57 pagesCholecystitis FinalRajendra DesaiNo ratings yet
- NCM-Ulcerative Colitis ReportDocument22 pagesNCM-Ulcerative Colitis ReportJocelyn RiveraNo ratings yet
- IBD - Shane Ryan ApperleyDocument63 pagesIBD - Shane Ryan Apperleyvivi avisaNo ratings yet
- 25 45 Disease That Result From The Malfunction of The Cell Cycle During Cell DivisionDocument20 pages25 45 Disease That Result From The Malfunction of The Cell Cycle During Cell DivisionathenazaharabautistaNo ratings yet
- Ibd AnushaDocument32 pagesIbd AnushaRupesh R100% (1)
- Acute Abdomen: Physiology, Evaluation and DDXDocument87 pagesAcute Abdomen: Physiology, Evaluation and DDXDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- IBD-Rough Road - Case Study in IBD From Presentation To ManagementDocument4 pagesIBD-Rough Road - Case Study in IBD From Presentation To ManagementBejan CorinaNo ratings yet
- Perforated Peptic UlcerDocument68 pagesPerforated Peptic UlcerSaibo BoldsaikhanNo ratings yet
- CSS Ulcerative ColitisDocument28 pagesCSS Ulcerative ColitisAthiyyah HasnaNo ratings yet
- IBD Final11Document41 pagesIBD Final11abraham debebeNo ratings yet
- DefinitionDocument12 pagesDefinitionAylol 23No ratings yet
- Jejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of LiteratureDocument6 pagesJejunojejunal Intussusception As Initial Presentation of Coeliac Disease: A Case Report and Review of Literatureellya theresiaNo ratings yet
- Perforated Peptic Ulcer Dr. Anbiar Manjas, SP.B-KBDDocument68 pagesPerforated Peptic Ulcer Dr. Anbiar Manjas, SP.B-KBDAndy YusufNo ratings yet
- Lecture 2-Part 1Document90 pagesLecture 2-Part 1mashe1No ratings yet
- A Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportDocument4 pagesA Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportAbdullah KhanNo ratings yet
- C. A Patient Who Withdraw Normally, But Can't Localize A Painful Stimuli, Has A Score of 5 On Motor Response Part of Glasgow Coma ScaleDocument13 pagesC. A Patient Who Withdraw Normally, But Can't Localize A Painful Stimuli, Has A Score of 5 On Motor Response Part of Glasgow Coma ScaleDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Q 9Document39 pagesQ 9Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- ST NDDocument5 pagesST NDDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Q 2Document8 pagesQ 2Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- in The Workup On A Patient For Possible Appendicitis, CT Scanning Should Be PerformedDocument9 pagesin The Workup On A Patient For Possible Appendicitis, CT Scanning Should Be PerformedDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Q 4Document14 pagesQ 4Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- General Surgery Exam 6 /6/2020: Email Address Name and Number (English)Document8 pagesGeneral Surgery Exam 6 /6/2020: Email Address Name and Number (English)Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Untitled PageDocument1 pageUntitled PageDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Lung Disease PicsDocument169 pagesLung Disease PicsDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- De VIRGILIO-10Document36 pagesDe VIRGILIO-10Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Untitled PageDocument1 pageUntitled PageDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Bone Studing FileDocument42 pagesBone Studing FileDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Null 8Document6 pagesNull 8Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Untitled PageDocument1 pageUntitled PageDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Finger Tip InjuryDocument46 pagesFinger Tip InjuryDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Soft Tissue PicDocument132 pagesSoft Tissue PicDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- امتحان سنة ثالثة 2023Document15 pagesامتحان سنة ثالثة 2023Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Null 9Document3 pagesNull 9Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Neuro ReviweDocument2 pagesNeuro ReviweDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Facial ReconstructionDocument77 pagesFacial ReconstructionDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Pseudomembranous ColitisDocument39 pagesPseudomembranous ColitisDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Incisional HerniaDocument48 pagesIncisional HerniaDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Pediatric Neck Masses, TEF, Diaphragmatic HerniaDocument101 pagesPediatric Neck Masses, TEF, Diaphragmatic HerniaDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Atypical Colorectal NeoplasmsDocument52 pagesAtypical Colorectal NeoplasmsDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Board ReviewDocument24 pagesBoard ReviewDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- OpioidsDocument35 pagesOpioidsDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- BreastDocument90 pagesBreastDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Escharotomies and Fasciotomies Operative SessionDocument31 pagesEscharotomies and Fasciotomies Operative SessionDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Hernias: Types, Diagnosis, Management and ComplicationsDocument134 pagesHernias: Types, Diagnosis, Management and ComplicationsDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- HerniaDocument106 pagesHerniaDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Sutent Epar Risk Management Plan Summary - enDocument7 pagesSutent Epar Risk Management Plan Summary - enAna MariaNo ratings yet
- Sympatholytic DrugsDocument8 pagesSympatholytic DrugsJianne CaloNo ratings yet
- Android Based Expert System Application For Diagnose COVID-19 Disease Cases Study of Banyumas RegencyDocument14 pagesAndroid Based Expert System Application For Diagnose COVID-19 Disease Cases Study of Banyumas RegencyEbenezer OgidioluNo ratings yet
- Micu CasesDocument2 pagesMicu CasesDinarkram Rabreca EculNo ratings yet
- Diphtheria: Sabah Mohsin Al-Maamuri MDDocument3 pagesDiphtheria: Sabah Mohsin Al-Maamuri MDAmmar AlnajjarNo ratings yet
- HIV AIDS Workplace Policy ProgramDocument4 pagesHIV AIDS Workplace Policy ProgramLauro CanceranNo ratings yet
- EmphysemaDocument27 pagesEmphysemaDiana Laura LeiNo ratings yet
- Soal MCQ USU 2009Document19 pagesSoal MCQ USU 2009SuzetteNo ratings yet
- FILE 28 June QDocument45 pagesFILE 28 June QHanan HejaziNo ratings yet
- Case Study Final OutputDocument42 pagesCase Study Final Outputroizen bagamaspadNo ratings yet
- Herbal Antibiotics 1999 - BuhnerDocument676 pagesHerbal Antibiotics 1999 - BuhnerJoyce-Bea Vu50% (4)
- Homoeopathic Management of Lumbar Disc ProlapseDocument5 pagesHomoeopathic Management of Lumbar Disc ProlapsessalmahfuzNo ratings yet
- Allergic Rhinitis: PathophysiologyDocument28 pagesAllergic Rhinitis: Pathophysiologysneh1509No ratings yet
- Arthritis 1Document25 pagesArthritis 1NOORUDDINNo ratings yet
- Mental Health & Prevention: Ruth Mcintyre, Patrick Smith, Katharine A. RimesDocument15 pagesMental Health & Prevention: Ruth Mcintyre, Patrick Smith, Katharine A. RimesbooksrgoodNo ratings yet
- Complex Care For Nursing Questions and AnswersDocument15 pagesComplex Care For Nursing Questions and Answerslayla kambala100% (1)
- Diabetic NeuropathyDocument13 pagesDiabetic NeuropathyFatima MehboobNo ratings yet
- AntibioticsDocument4 pagesAntibioticsVladimir GurjanovNo ratings yet
- IgG4 Related DiseaseDocument12 pagesIgG4 Related DiseaseSofia SimpertigueNo ratings yet
- Trans 4 Malignant Proliferations of The Skin DR GuillanoDocument7 pagesTrans 4 Malignant Proliferations of The Skin DR GuillanofredrrgNo ratings yet
- Postural DrainageDocument13 pagesPostural DrainageSalman KhanNo ratings yet
- Febra La Pacientul Imunodeprimat (Romana)Document59 pagesFebra La Pacientul Imunodeprimat (Romana)ialomitaNo ratings yet
- Why You Will Need A Silencil Consumer Testimonialsogxbp PDFDocument3 pagesWhy You Will Need A Silencil Consumer Testimonialsogxbp PDFchungtrolle48No ratings yet
- General Biology I M5Document20 pagesGeneral Biology I M5Anjhiene CambaNo ratings yet
- Disorders PDFDocument2 pagesDisorders PDFsamNo ratings yet
- Simple Genetics - A Guided InquiryDocument3 pagesSimple Genetics - A Guided InquiryElijah ExumNo ratings yet
- Fcs 402-Mini Case StudyDocument13 pagesFcs 402-Mini Case Studyapi-609685665No ratings yet
- Creatina y CerebroDocument16 pagesCreatina y CerebroAlberto ValenzuelaNo ratings yet
- Quiz 12 AnswersDocument3 pagesQuiz 12 AnswersAllah YarNo ratings yet