You might also like
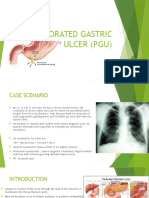
- Perforated Gastric Ulcer (Pgu)Document10 pagesPerforated Gastric Ulcer (Pgu)Jen NeeNo ratings yet
- IBDDocument27 pagesIBDKatarina SilalahiNo ratings yet
- Practical Algorithms in Pediatric Gastroenterology: EditorDocument116 pagesPractical Algorithms in Pediatric Gastroenterology: EditorandresNo ratings yet
- Scintigraphicdetectionof Segmentalbile-Ductobstruction: Case ReportsDocument2 pagesScintigraphicdetectionof Segmentalbile-Ductobstruction: Case ReportsMuzafar AhmedNo ratings yet
- Rupture of A Hydatid Cyst Into The Bile DuctDocument3 pagesRupture of A Hydatid Cyst Into The Bile DuctasclepiuspdfsNo ratings yet
- Diagnosis and Management of Hepatolithiasis in An.242Document4 pagesDiagnosis and Management of Hepatolithiasis in An.242Mike ChristantiNo ratings yet
- Carol I SyndromeDocument3 pagesCarol I SyndromefebrymaharaniputriNo ratings yet
- Hepatolithiasis May Increase Risk of CholangiocarcinomaDocument4 pagesHepatolithiasis May Increase Risk of CholangiocarcinomaNurul RifqianiNo ratings yet
- En V25n1a22Document4 pagesEn V25n1a22Alexandre AlexandreNo ratings yet
- GallbladderDocument44 pagesGallbladderAli SafaaNo ratings yet
- Pathogenesis and Management of Hepatolithiasis: A Report of Two CasesDocument3 pagesPathogenesis and Management of Hepatolithiasis: A Report of Two CasesBenny KurniawanNo ratings yet
- Gallbladder VolulusDocument5 pagesGallbladder Volulusalexandra.calorNo ratings yet
- Complex Case of Ureteropelvic Junction Obstruction 2024 International JournaDocument3 pagesComplex Case of Ureteropelvic Junction Obstruction 2024 International JournaRonald QuezadaNo ratings yet
- Anomalous Non-bifurcating Portal Vein Protected During Extended Right Hepatectomy Using Hanging ManeuverDocument7 pagesAnomalous Non-bifurcating Portal Vein Protected During Extended Right Hepatectomy Using Hanging ManeuverMARIO DCARLO TREJO HUAMANNo ratings yet
- International Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. AwasthiDocument3 pagesInternational Journal of Infectious Diseases: Anshuman Pandey, Shakeel Masood, Namrata P. Awasthijohanna monsalveNo ratings yet
- At Two: Was SeDocument3 pagesAt Two: Was Seida ayu agung WijayantiNo ratings yet
- Incidentally Exploration of The Fusiform Cystic Duct 2024 International JourDocument4 pagesIncidentally Exploration of The Fusiform Cystic Duct 2024 International JourRonald QuezadaNo ratings yet
- Biliary Ileus A Case Report With A Brief ReviewDocument5 pagesBiliary Ileus A Case Report With A Brief ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Acute Median Arcuate Ligament Syndrome After PancreaticoduodenectomyDocument5 pagesAcute Median Arcuate Ligament Syndrome After PancreaticoduodenectomyAna Karen RNo ratings yet
- Post LapChole Bile LeaksDocument41 pagesPost LapChole Bile LeaksIfeanyichukwu OgbonnayaNo ratings yet
- Absence of The Cystic Duct:: A Case Report, A Review of LiteratureDocument3 pagesAbsence of The Cystic Duct:: A Case Report, A Review of LiteratureBolivar IseaNo ratings yet
- EN Acute Pancreatitis As A Complication ofDocument5 pagesEN Acute Pancreatitis As A Complication ofShandy JonnerNo ratings yet
- CEJoU4 str273-275Document3 pagesCEJoU4 str273-275chelseareynaNo ratings yet
- Hepatic Subcapsular BIloma A Rare Complication of Laparoscopic CholecystectomyDocument4 pagesHepatic Subcapsular BIloma A Rare Complication of Laparoscopic CholecystectomyIndra PrimaNo ratings yet
- Intraductal Papillary Neoplasm of the Bile Duct Case ReportDocument5 pagesIntraductal Papillary Neoplasm of the Bile Duct Case ReportFernando SousaNo ratings yet
- Liver Disease: Schwartz Principles of Surgery2010Document50 pagesLiver Disease: Schwartz Principles of Surgery2010ralphNo ratings yet
- Choledochal Cyst: SymposiumDocument3 pagesCholedochal Cyst: SymposiumRegi Anastasya MangiriNo ratings yet
- TMP CD3Document4 pagesTMP CD3FrontiersNo ratings yet
- Z - 2009-08 - Pancreatic Pseudocyst With Pancreatolithiasis and Intracystic Hemorrhage Treated With Distal Pancreatectomy - A Case ReportDocument5 pagesZ - 2009-08 - Pancreatic Pseudocyst With Pancreatolithiasis and Intracystic Hemorrhage Treated With Distal Pancreatectomy - A Case ReportNawzad SulayvaniNo ratings yet
- 19Document3 pages19Elizabeth ToapantaNo ratings yet
- Surgery - Liver Part 1Document9 pagesSurgery - Liver Part 1wedikaf807No ratings yet
- The Radiology Assistant - Biliary Duct PathologyDocument34 pagesThe Radiology Assistant - Biliary Duct Pathologycarlasimonetti92No ratings yet
- Normal Anatomic VariantDocument13 pagesNormal Anatomic VariantNatnael GetahunNo ratings yet
- Beware Left-Sided Gallbladder (LSGBDocument2 pagesBeware Left-Sided Gallbladder (LSGBLidiaNo ratings yet
- Cystic Duct Remnant Syndrome: Myth or Reality?: Sı Ndrome Del Mun o N Cı Stico: Quimera o Realidad?Document2 pagesCystic Duct Remnant Syndrome: Myth or Reality?: Sı Ndrome Del Mun o N Cı Stico: Quimera o Realidad?Mirkops CruzNo ratings yet
- Obstructive Jaundice A Clinical StudyDocument7 pagesObstructive Jaundice A Clinical StudyAnisah Maryam DianahNo ratings yet
- Management of Accessory Hepatic Ducts in Choledochal CystsDocument2 pagesManagement of Accessory Hepatic Ducts in Choledochal CystsJosé MartínezNo ratings yet
- Biliary Cast Syndrome in Portal Hypertensive Biliopathy: Direct Cholangioscopic Findings and Endoscopic Therapy With Metal StentDocument3 pagesBiliary Cast Syndrome in Portal Hypertensive Biliopathy: Direct Cholangioscopic Findings and Endoscopic Therapy With Metal StentMarcelo CalossoNo ratings yet
- Chist ColedocDocument7 pagesChist ColedocAlina MihuNo ratings yet
- 2018-10 - Ischemic Cholangiopathy 11 Years After Liver Transplantation From Asymptomatic Chronic Hepatic Artery ThrombosisDocument3 pages2018-10 - Ischemic Cholangiopathy 11 Years After Liver Transplantation From Asymptomatic Chronic Hepatic Artery ThrombosisNawzad SulayvaniNo ratings yet
- Bile Leaks After Laparoscopic CholecystectomyDocument25 pagesBile Leaks After Laparoscopic CholecystectomyPinky NairNo ratings yet
- Duplication of Gallbladder: Case ReportDocument3 pagesDuplication of Gallbladder: Case ReportVenanda RianNo ratings yet
- Bile LeakDocument3 pagesBile LeakraghavagummadiNo ratings yet
- Triple GallbladerDocument12 pagesTriple GallbladerRudy Arindra WijayaNo ratings yet
- Liver and BiliaryDocument15 pagesLiver and Biliaryasmatmasoom5566No ratings yet
- Case Report - CholesystitisDocument4 pagesCase Report - CholesystitisBenzoyl BeingNo ratings yet
- Pancreatic Adenocarcinoma Mimicking PseudocystDocument3 pagesPancreatic Adenocarcinoma Mimicking PseudocystInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Severe Complications of Chronic Cholelithiasis TreatmentDocument8 pagesSevere Complications of Chronic Cholelithiasis Treatmentabraham suarezNo ratings yet
- 54.the Gallbladder and Bile DuctsDocument19 pages54.the Gallbladder and Bile DuctsAdenegan Adesola RaymondNo ratings yet
- Kolangitis Case 1Document6 pagesKolangitis Case 1Dhen Mas PrimanaNo ratings yet
- HydronephrosisDocument3 pagesHydronephrosisCarla AlmerolNo ratings yet
- Jurnal 2Document10 pagesJurnal 2Siska Eni WijayantiNo ratings yet
- Ladd's Band in The Adult, An Unusual Case of Occlusion Case Report Andreview of The LiteratureDocument5 pagesLadd's Band in The Adult, An Unusual Case of Occlusion Case Report Andreview of The Literaturewaldemar russellNo ratings yet
- Iatrogenic Injury To The Common Bile Duct: Case ReportDocument3 pagesIatrogenic Injury To The Common Bile Duct: Case ReportGianfranco MuntoniNo ratings yet
- Insignis Surgery 2 Gallbladder and Extrahepatic Biliary SystemDocument7 pagesInsignis Surgery 2 Gallbladder and Extrahepatic Biliary SystemPARADISE JanoNo ratings yet
- Biliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou UniversityDocument75 pagesBiliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou Universityapi-19916399No ratings yet
- Bile Leakage During Laparoscopic Cholecystectomy A Rare Case of Aberrant AnatomyDocument6 pagesBile Leakage During Laparoscopic Cholecystectomy A Rare Case of Aberrant AnatomyEditor IJTSRDNo ratings yet
- IVC Leiomyosarcoma Reconstruction Not Always RequiredDocument3 pagesIVC Leiomyosarcoma Reconstruction Not Always RequiredCirugía General Hospital de San JoséNo ratings yet
- s13304 011 0131 2 PDFDocument3 pagess13304 011 0131 2 PDFRoderick Núñez JNo ratings yet
- The Diagnosis and Management of Gallstones in The Elderly: Liver DiseasesDocument5 pagesThe Diagnosis and Management of Gallstones in The Elderly: Liver Diseasessusanto kusumaNo ratings yet
- Retroperitoneal Hydatid Cyst Challenging The Dia - 2024 - International JournalDocument4 pagesRetroperitoneal Hydatid Cyst Challenging The Dia - 2024 - International JournalRonald QuezadaNo ratings yet
- Case Report of Ectopic Hepatic Tissue, A Rare Finding DuringDocument4 pagesCase Report of Ectopic Hepatic Tissue, A Rare Finding DuringAnila CakeNo ratings yet
- Nuclear-MedicineDocument54 pagesNuclear-Medicinesuraj rajpurohitNo ratings yet
- STM Kolkata History (1)Document45 pagesSTM Kolkata History (1)suraj rajpurohitNo ratings yet
- GUILLAIN-BARRE SYNDROME (1)Document42 pagesGUILLAIN-BARRE SYNDROME (1)suraj rajpurohitNo ratings yet
- ASH VTE Guidelines - Snapshot - 1PGR - VTE - PEDocument1 pageASH VTE Guidelines - Snapshot - 1PGR - VTE - PEAzka FuadyNo ratings yet
- Esophageal diseases and surgical managementDocument72 pagesEsophageal diseases and surgical managementBiniamNo ratings yet
- Komplikasi Operasi HemorrhoidDocument28 pagesKomplikasi Operasi HemorrhoidVelrones TampubolonNo ratings yet
- Hischsprug Disease by HamadDocument31 pagesHischsprug Disease by HamadALIEF MUTHIANo ratings yet
- Case Presentation About Calculous CholecyctitisDocument23 pagesCase Presentation About Calculous CholecyctitiskarenNo ratings yet
- IBS ResearchDocument2 pagesIBS ResearchDrHassan Ahmed ShaikhNo ratings yet
- AJEERNA (Indigestion)Document37 pagesAJEERNA (Indigestion)m gouriNo ratings yet
- List of Common Digestive DiseasesDocument25 pagesList of Common Digestive DiseasesKristeine LimNo ratings yet
- Abdominal PainDocument7 pagesAbdominal PainKartikey ChauhanNo ratings yet
- Drug StudyDocument5 pagesDrug StudyGAYOL BREEN IRAH A.No ratings yet
- Emilok 2011 MKT Plan TOTAL2Document19 pagesEmilok 2011 MKT Plan TOTAL2maawi2002yahoocomNo ratings yet
- The Gastro-Intestinal SystemDocument12 pagesThe Gastro-Intestinal SystemRenelyn ComiaNo ratings yet
- HepatobiliaryDocument22 pagesHepatobiliarypaulandtess27No ratings yet
- MS Sas 7Document4 pagesMS Sas 7rereNo ratings yet
- SenokotDocument1 pageSenokotKatie McPeek100% (1)
- Acute and Chronic GastritisDocument17 pagesAcute and Chronic GastritisIndah Nur PratiwiNo ratings yet
- Gastro - NelsonDocument14 pagesGastro - NelsonGemma OrquioNo ratings yet
- Diseases of OesophagusDocument46 pagesDiseases of OesophagusBrother GeorgeNo ratings yet
- Jurnal Pengobatan GastritisDocument7 pagesJurnal Pengobatan Gastritisnana kuna100% (1)
- Abdominal Assessment GuideDocument2 pagesAbdominal Assessment GuidepriyaNo ratings yet
- Acute Abdominal PainDocument2 pagesAcute Abdominal PainWinnieNo ratings yet
- Book 1Document166 pagesBook 1Puput HepitasariNo ratings yet
- GERDDocument32 pagesGERDlumina.sNo ratings yet
- HANDOUT - Vomiting in AdultsDocument3 pagesHANDOUT - Vomiting in Adults2012No ratings yet
- Pancreatic Cancer Symptoms and Diagnosis - Google SearchDocument3 pagesPancreatic Cancer Symptoms and Diagnosis - Google Searchranjit__kayalaNo ratings yet
- Median Rhomboid GlossitisDocument7 pagesMedian Rhomboid Glossitisshahzeb memonNo ratings yet
- Intestinal ObstructionDocument157 pagesIntestinal ObstructionOmar SuleimanNo ratings yet
- Williamson CasestudyDocument31 pagesWilliamson Casestudyapi-369065120No ratings yet