You might also like
- LMA Van Der Velden PDFDocument88 pagesLMA Van Der Velden PDFKarla Novoa PérezNo ratings yet
- Solastra Tech Spec Sheet BrochureDocument5 pagesSolastra Tech Spec Sheet BrochurecandiddreamsNo ratings yet
- Minimal Residual Disease - PGPDocument76 pagesMinimal Residual Disease - PGPabhinav_choudhary03No ratings yet
- Craig Chronic Lymphoid Disorders Useful Information CCEN India 2018 FinalDocument9 pagesCraig Chronic Lymphoid Disorders Useful Information CCEN India 2018 FinalBrahmananda ChakrabortyNo ratings yet
- 03 - Approach Hematolymphoid NeoplasmsDocument119 pages03 - Approach Hematolymphoid NeoplasmscandiddreamsNo ratings yet
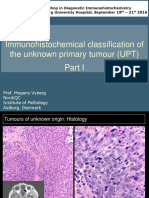
- Immunohistochemical Classification of The Unknown Primary Tumour (UPT)Document87 pagesImmunohistochemical Classification of The Unknown Primary Tumour (UPT)Abhugz VosotrosNo ratings yet
- Immunophenotyping - An Introduction by Brig Tahir Aziz AhmedDocument65 pagesImmunophenotyping - An Introduction by Brig Tahir Aziz AhmedOmair RiazNo ratings yet
- EuroFlow Ab Panels and Technical Information - Version 1.10Document14 pagesEuroFlow Ab Panels and Technical Information - Version 1.10Jéssica ParenteNo ratings yet
- An Interesting Hematopathology Case: Christopher Julien PGY2Document41 pagesAn Interesting Hematopathology Case: Christopher Julien PGY2Christopher JulienNo ratings yet
- EBVv CaseDocument9 pagesEBVv CaseJason SteelNo ratings yet
- BD OneFlow ALOT IFU EUDocument50 pagesBD OneFlow ALOT IFU EUlam sẽNo ratings yet
- Chronic Lymphocytic Leukemia (CLL) : Curs An IV - Limba Engleza 2012-2013Document49 pagesChronic Lymphocytic Leukemia (CLL) : Curs An IV - Limba Engleza 2012-2013Tresor MbuyiNo ratings yet
- Review of Peripheral Blood and Bone Marrow Malignant DiseaseDocument112 pagesReview of Peripheral Blood and Bone Marrow Malignant DiseaseashjanbaslaibNo ratings yet
- Abstrak MURNIATI PosterDocument5 pagesAbstrak MURNIATI PosterMohammad Rosyid RidhoNo ratings yet
- Osteogenic Differentiation and Analysis of MSC: Application NoteDocument5 pagesOsteogenic Differentiation and Analysis of MSC: Application NotednnfdaNo ratings yet
- B&T Cell Clonality PDFDocument22 pagesB&T Cell Clonality PDFKarla Novoa PérezNo ratings yet
- 06 Flow Cytometry in Diagnosis of ALLDocument30 pages06 Flow Cytometry in Diagnosis of ALLcandiddreamsNo ratings yet
- FlowDocument85 pagesFlowShephali SharmaNo ratings yet
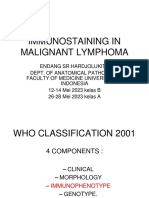
- Immunostaining in Malignant Lymphoma Kelas BDocument40 pagesImmunostaining in Malignant Lymphoma Kelas BZuhri MardiahNo ratings yet
- Haematology AnalyzerDocument10 pagesHaematology AnalyzerharrisshaikhNo ratings yet
- Hematology Discussion 2011 KPBDocument10 pagesHematology Discussion 2011 KPBtufis02No ratings yet
- CCV1 FCDocument2 pagesCCV1 FCaminata6No ratings yet
- A Guide To Human Immune Cell Characterization by Flow CytometryDocument5 pagesA Guide To Human Immune Cell Characterization by Flow CytometryLeo TolstoyNo ratings yet
- Flow Cytometry - Beyond CD4Document99 pagesFlow Cytometry - Beyond CD4joanne.luider753No ratings yet
- 1-What Is Leukemia?Document4 pages1-What Is Leukemia?نواف الزهرانيNo ratings yet
- PDFDocument86 pagesPDFXuan TuanNo ratings yet
- 5 Challenge Case Workbook and DiscussionDocument17 pages5 Challenge Case Workbook and DiscussionBrahmananda ChakrabortyNo ratings yet
- Kuliah LeukimiaDocument31 pagesKuliah LeukimiaMohammad SutamiNo ratings yet
- Morphologic and Location-Based Classifi Cation of Differentiating Erythroid Lineage Cells Using The ImagestreamDocument4 pagesMorphologic and Location-Based Classifi Cation of Differentiating Erythroid Lineage Cells Using The ImagestreamNeeraj KannaugiyaNo ratings yet
- AML Pita DR MardiahDocument71 pagesAML Pita DR MardiahSarly Puspita AriesaNo ratings yet
- Composition of EuroFlow Panels and Technical Information On Reagents Version 1.4Document14 pagesComposition of EuroFlow Panels and Technical Information On Reagents Version 1.4Liliana SolariNo ratings yet
- He Ma To Pathology Sample ReportDocument7 pagesHe Ma To Pathology Sample ReportPavel Nesmiyanov100% (1)
- Manual of Diagnostic Antibodies For Immunohistology - 1841101001Document539 pagesManual of Diagnostic Antibodies For Immunohistology - 1841101001dudapaskasNo ratings yet
- Flow Cytometric Analysis of Lymphomas: Current Status and UsefulnessDocument9 pagesFlow Cytometric Analysis of Lymphomas: Current Status and Usefulnessসোমনাথ মহাপাত্রNo ratings yet
- 1212g in HematologyDocument11 pages1212g in HematologyHarika PutraNo ratings yet
- ადამიანის CD ანტიგენებიDocument1 pageადამიანის CD ანტიგენებიEMD GROUP100% (1)
- Case 5 Workbook and DiscussionDocument14 pagesCase 5 Workbook and DiscussionBrahmananda ChakrabortyNo ratings yet
- EAHP With Corrections (V2) - Changes by GCC (On 10-4-19)Document2 pagesEAHP With Corrections (V2) - Changes by GCC (On 10-4-19)Christopher JulienNo ratings yet
- EUROFLOW ANTIBODY PANELS Cytognos BrochureDocument1 pageEUROFLOW ANTIBODY PANELS Cytognos Brochure82lauNo ratings yet
- KJM 2022 97 5 308Document11 pagesKJM 2022 97 5 308knighderNo ratings yet
- 1.6+7 Laboratory Investigation and Film Interpretation WITH ANSWERSDocument34 pages1.6+7 Laboratory Investigation and Film Interpretation WITH ANSWERSAlex KamougerosNo ratings yet
- Immunophenotyping: Myeloid Cell Maturation: Bone MarrowDocument2 pagesImmunophenotyping: Myeloid Cell Maturation: Bone Marrowapi-168505054No ratings yet
- Hematology Interest Group CNL Myeloproliferative NeoplasmDocument10 pagesHematology Interest Group CNL Myeloproliferative Neoplasmapi-384537137No ratings yet
- HematopoieticDocument1 pageHematopoieticborsk8674No ratings yet
- 1.6+7 Laboratory Investigation and Film Interpretation WITHOUT ANSWERSDocument21 pages1.6+7 Laboratory Investigation and Film Interpretation WITHOUT ANSWERSAlex KamougerosNo ratings yet
- BoardReviewPart2B MalignantHemePathDocument207 pagesBoardReviewPart2B MalignantHemePathMaria Cristina Alarcon NietoNo ratings yet
- Mr. S/67 Yo/bengawan Solo WardDocument27 pagesMr. S/67 Yo/bengawan Solo WardMuhammad BilalNo ratings yet
- ASH Hematology Review Series - CAR-T Porter Sub 8-5-21Document63 pagesASH Hematology Review Series - CAR-T Porter Sub 8-5-21Иван НегарэNo ratings yet
- Gujral FCMDocument102 pagesGujral FCMcandiddreamsNo ratings yet
- Lymphocytic Leukemia in A Golden Retriever Dog - A CaseDocument14 pagesLymphocytic Leukemia in A Golden Retriever Dog - A CaseGanesh DasaraNo ratings yet
- Blood Cell Formation and Blood CellsDocument49 pagesBlood Cell Formation and Blood Cellsxcx88igNo ratings yet
- Lab Activity No. 5 - Slide PresentationDocument24 pagesLab Activity No. 5 - Slide PresentationChelsea Padilla Delos ReyesNo ratings yet
- Cardiovascular System:The Blood - NSUDocument47 pagesCardiovascular System:The Blood - NSUGregrodockerNo ratings yet
- Answers - Haematological Malignancies Digital Images QuizDocument4 pagesAnswers - Haematological Malignancies Digital Images Quizcande casanasNo ratings yet
- Lymphocytic Leukemia in A Golden Retriever Dog - A Case ReportDocument14 pagesLymphocytic Leukemia in A Golden Retriever Dog - A Case ReportGanesh DasaraNo ratings yet
- Leukemia SOPDocument8 pagesLeukemia SOPBrahmananda ChakrabortyNo ratings yet
- Diagnostic Usefulness and Prognostic Impact of CD200 Expression in Lymphoid Malignancies and Plasma Cell MyelomaDocument8 pagesDiagnostic Usefulness and Prognostic Impact of CD200 Expression in Lymphoid Malignancies and Plasma Cell MyelomaBrahma AcharNo ratings yet
- Chronic Itp - Karen Nina Ocampo 09012008Document61 pagesChronic Itp - Karen Nina Ocampo 09012008LIMRA ALAMNo ratings yet
- Casos Clinicos de Hematopatología IiDocument5 pagesCasos Clinicos de Hematopatología IiRicardo LaraNo ratings yet
- STI/RTI Syndromic Case Management - NACODocument1 pageSTI/RTI Syndromic Case Management - NACOTejas100% (8)
- Quiz 02 HPB, PancreasDocument11 pagesQuiz 02 HPB, Pancreasimran khanNo ratings yet
- Recalled Neet pg2023Document7 pagesRecalled Neet pg2023imran khanNo ratings yet
- Provisional State Merit ListDocument101 pagesProvisional State Merit Listimran khanNo ratings yet
- STI/RTI Syndromic Case Management - NACODocument1 pageSTI/RTI Syndromic Case Management - NACOTejas100% (8)
- Iap Sms Textbook of Community MedicineDocument2 pagesIap Sms Textbook of Community Medicineimran khanNo ratings yet
- Comparison of Two Different Methods of Detecting Residual CariesDocument6 pagesComparison of Two Different Methods of Detecting Residual Cariesimran khanNo ratings yet
- Delayed Photoactivation of Dualcure Composites Effect On Cuspal Flexure, Depth-Of-cure, and Mechanical PropertiesDocument8 pagesDelayed Photoactivation of Dualcure Composites Effect On Cuspal Flexure, Depth-Of-cure, and Mechanical Propertiesimran khanNo ratings yet
- NEWSLETTER-D-Dimer & Its Use in COVID 19Document5 pagesNEWSLETTER-D-Dimer & Its Use in COVID 19imran khanNo ratings yet
- Endodontic and Clinical Considerations in The Management of Variable Anatomy in Mandibular Premolars A Literature ReviewDocument12 pagesEndodontic and Clinical Considerations in The Management of Variable Anatomy in Mandibular Premolars A Literature Reviewimran khanNo ratings yet
- Effect of ProTaper and Reciproc Preparation and Gutta-Percha Cone On Cold Lateral CompactionDocument7 pagesEffect of ProTaper and Reciproc Preparation and Gutta-Percha Cone On Cold Lateral Compactionimran khanNo ratings yet
- The Internal Root Canal Morphology of Single Rooted Mandibular Canines Revealed by Micro ComputedDocument4 pagesThe Internal Root Canal Morphology of Single Rooted Mandibular Canines Revealed by Micro Computedimran khanNo ratings yet
- NEWSLETTER-D-Dimer & Its Use in COVID 19Document5 pagesNEWSLETTER-D-Dimer & Its Use in COVID 19imran khanNo ratings yet
- Reminova and EAER Keeping Enamel Whole Through Caries RemineralizationDocument7 pagesReminova and EAER Keeping Enamel Whole Through Caries Remineralizationimran khanNo ratings yet
- Comparison of The Fracture Resistance of Three Different Recent Composite Systems in Large Class II Mesio-Occlusal Distal Cavities An in Vitro StudyDocument5 pagesComparison of The Fracture Resistance of Three Different Recent Composite Systems in Large Class II Mesio-Occlusal Distal Cavities An in Vitro Studyimran khanNo ratings yet
- The Internal Root Canal Morphology of Single Rooted Mandibular Canines Revealed by Micro ComputedDocument4 pagesThe Internal Root Canal Morphology of Single Rooted Mandibular Canines Revealed by Micro Computedimran khanNo ratings yet
- Comparison of The Fracture Resistance of Three Different Recent Composite Systems in Large Class II Mesio-Occlusal Distal Cavities An in Vitro StudyDocument5 pagesComparison of The Fracture Resistance of Three Different Recent Composite Systems in Large Class II Mesio-Occlusal Distal Cavities An in Vitro Studyimran khanNo ratings yet
- New Ultrasonic Tip Decreases Uninstrumented Surface andDocument7 pagesNew Ultrasonic Tip Decreases Uninstrumented Surface andimran khanNo ratings yet
- Impact of Contracted Endodontic Cavities On Root Canal Disinfection and Shaping PDFDocument7 pagesImpact of Contracted Endodontic Cavities On Root Canal Disinfection and Shaping PDFSoleyliLizbhetNo ratings yet
- Incidence of Middle Mesial Canals Based On Distance Between Mesial Canal Orifices in Mandibular Molars A Clinical and Cone-Beam Computed Tomographic AnalysisDocument4 pagesIncidence of Middle Mesial Canals Based On Distance Between Mesial Canal Orifices in Mandibular Molars A Clinical and Cone-Beam Computed Tomographic Analysisimran khanNo ratings yet
- Clindamycin Drug DeliveryDocument8 pagesClindamycin Drug DeliveryShaliniNo ratings yet
- New Ultrasonic Tip Decreases Uninstrumented Surface andDocument7 pagesNew Ultrasonic Tip Decreases Uninstrumented Surface andimran khanNo ratings yet
- Comparison of The Fracture Resistance of Three Different Recent Composite Systems in Large Class II Mesio-Occlusal Distal Cavities An in Vitro StudyDocument5 pagesComparison of The Fracture Resistance of Three Different Recent Composite Systems in Large Class II Mesio-Occlusal Distal Cavities An in Vitro Studyimran khanNo ratings yet
- Delayed Photoactivation of Dualcure Composites Effect On Cuspal Flexure, Depth-Of-cure, and Mechanical PropertiesDocument8 pagesDelayed Photoactivation of Dualcure Composites Effect On Cuspal Flexure, Depth-Of-cure, and Mechanical Propertiesimran khanNo ratings yet
- Incidence of Middle Mesial Canals Based On Distance Between Mesial Canal Orifices in Mandibular Molars A Clinical and Cone-Beam Computed Tomographic AnalysisDocument4 pagesIncidence of Middle Mesial Canals Based On Distance Between Mesial Canal Orifices in Mandibular Molars A Clinical and Cone-Beam Computed Tomographic Analysisimran khanNo ratings yet
- Impact of Contracted Endodontic Cavities On Root Canal Disinfection and Shaping PDFDocument7 pagesImpact of Contracted Endodontic Cavities On Root Canal Disinfection and Shaping PDFSoleyliLizbhetNo ratings yet
- Reminova and EAER Keeping Enamel Whole Through Caries RemineralizationDocument7 pagesReminova and EAER Keeping Enamel Whole Through Caries Remineralizationimran khanNo ratings yet
- Using QC BrochureDocument8 pagesUsing QC BrochureRizaNo ratings yet
- Lab Guide - Proficiency TestingDocument17 pagesLab Guide - Proficiency Testingimran khanNo ratings yet
- Support Vector Machine Master ThesisDocument7 pagesSupport Vector Machine Master Thesistammymajorsclarksville100% (2)
- Review Course 2 (Review On Professional Education Courses)Document8 pagesReview Course 2 (Review On Professional Education Courses)Regie MarcosNo ratings yet
- Ass AsDocument23 pagesAss AsMukesh BishtNo ratings yet
- Bassoon (FAGOT) : See AlsoDocument36 pagesBassoon (FAGOT) : See Alsocarlos tarancón0% (1)
- SRS For Travel AgencyDocument5 pagesSRS For Travel AgencyHardik SawalsaNo ratings yet
- Kaun Banega Crorepati Computer C++ ProjectDocument20 pagesKaun Banega Crorepati Computer C++ ProjectDhanya SudheerNo ratings yet
- Unit 20: TroubleshootingDocument12 pagesUnit 20: TroubleshootingDongjin LeeNo ratings yet
- S3 U4 MiniTestDocument3 pagesS3 U4 MiniTestĐinh Thị Thu HàNo ratings yet
- Hesychasm - A Christian Path of TranscendenceDocument10 pagesHesychasm - A Christian Path of Transcendencebde_gnas100% (1)
- CLT Apllications NewestDocument49 pagesCLT Apllications NewestMackBrideNo ratings yet
- M2252D PS PDFDocument36 pagesM2252D PS PDFCarmen da SilvaNo ratings yet
- ManualDocument24 pagesManualCristian ValenciaNo ratings yet
- Intercultural Personhood and Identity NegotiationDocument13 pagesIntercultural Personhood and Identity NegotiationJoão HorrNo ratings yet
- Project Analysis - M5 - MotorwayDocument6 pagesProject Analysis - M5 - MotorwayMuhammad Haroon ArshadNo ratings yet
- Citrus Information Kit-Update: Reprint - Information Current in 1998Document53 pagesCitrus Information Kit-Update: Reprint - Information Current in 1998hamsa sewakNo ratings yet
- Corrosion Performance of Mild Steel and GalvanizedDocument18 pagesCorrosion Performance of Mild Steel and GalvanizedNarasimha DvlNo ratings yet
- Aman Singh Rathore Prelms Strategy For UPSCDocument26 pagesAman Singh Rathore Prelms Strategy For UPSCNanju NNo ratings yet
- Pull Cord Switch JayashreeDocument1 pagePull Cord Switch JayashreeNCNo ratings yet
- Krishna TejaDocument71 pagesKrishna TejaHimanshu GaurNo ratings yet
- Construction Drawing: Legend Notes For Sanitary Piping Installation General Notes NotesDocument1 pageConstruction Drawing: Legend Notes For Sanitary Piping Installation General Notes NotesrajavelNo ratings yet
- 1 AlarmvalveDocument9 pages1 AlarmvalveAnandNo ratings yet
- DeadlocksDocument41 pagesDeadlocksSanjal DesaiNo ratings yet
- IoT Security Checklist Web 10 17 r1Document39 pagesIoT Security Checklist Web 10 17 r1SubinNo ratings yet
- Chapter 1 INTRODUCTION TO LITERATUREDocument4 pagesChapter 1 INTRODUCTION TO LITERATUREDominique TurlaNo ratings yet
- Half Yearly Examination, 2017-18: MathematicsDocument7 pagesHalf Yearly Examination, 2017-18: MathematicsSusanket DuttaNo ratings yet
- Chrysler CDS System - Bulletin2Document6 pagesChrysler CDS System - Bulletin2Martin Boiani100% (1)
- KM170, KM171, KM172, F3A21, F3A22: 3 SPEED FWD (Lock Up & Non Lock Up)Document4 pagesKM170, KM171, KM172, F3A21, F3A22: 3 SPEED FWD (Lock Up & Non Lock Up)krzysiek1975No ratings yet
- Final Lesson PlanDocument3 pagesFinal Lesson Planapi-510713019No ratings yet
- MCFKTP G3 S2 SC Number Pattern PuzzlesDocument5 pagesMCFKTP G3 S2 SC Number Pattern PuzzlesEric GoNo ratings yet
- Anykycaccount Com Product Payoneer Bank Account PDFDocument2 pagesAnykycaccount Com Product Payoneer Bank Account PDFAnykycaccountNo ratings yet