0% found this document useful (0 votes)
417 views4 pages# CT Head Scan NICE Algorithm 2023
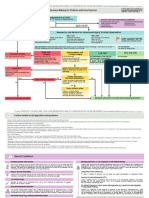
The document outlines algorithms for selecting people for CT head scans or imaging of the cervical spine following a head injury. It provides criteria for determining if a CT scan or imaging is needed based on factors like Glasgow Coma Scale scores, loss of consciousness, mechanism of injury, risk factors, and symptoms. The algorithms include multiple decision points and criteria for both adults and children.
Uploaded by
Belal HasanCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
417 views4 pages# CT Head Scan NICE Algorithm 2023
The document outlines algorithms for selecting people for CT head scans or imaging of the cervical spine following a head injury. It provides criteria for determining if a CT scan or imaging is needed based on factors like Glasgow Coma Scale scores, loss of consciousness, mechanism of injury, risk factors, and symptoms. The algorithms include multiple decision points and criteria for both adults and children.
Uploaded by
Belal HasanCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd