You might also like
- Carpal Tunnel Syndrome Questionnaire (CTSQ)Document1 pageCarpal Tunnel Syndrome Questionnaire (CTSQ)Samuel Iñiguez JiménezNo ratings yet
- DASHDocument2 pagesDASHNICOLE RAFAEL TACDERASNo ratings yet
- The English You Need for the Office: Business EnglishFrom EverandThe English You Need for the Office: Business EnglishRating: 4.5 out of 5 stars4.5/5 (9)
- DashDocument4 pagesDashjsyugesh21No ratings yet
- Boston Carpal Tunnel Questionnaire BCTSQDocument2 pagesBoston Carpal Tunnel Questionnaire BCTSQmario benjamin suarez carcamoNo ratings yet
- Let's Investigate! Hands-On Science - Grades 1-2From EverandLet's Investigate! Hands-On Science - Grades 1-2Rating: 5 out of 5 stars5/5 (1)
- Quickdash: Quickdash Disability/Symptom Score (Sum of N Responses) - 1 X 25Document1 pageQuickdash: Quickdash Disability/Symptom Score (Sum of N Responses) - 1 X 25Louise AxalanNo ratings yet
- Unsinkable Sub, The: Ready-Made Lessons for Last-Minute DaysFrom EverandUnsinkable Sub, The: Ready-Made Lessons for Last-Minute DaysNo ratings yet
- DashDocument1 pageDashKathryn LasNo ratings yet
- DASHDocument3 pagesDASHLily Ann D. BautistaNo ratings yet
- Boston Carpal Tunnel Syndrome Questionnaire (BCTQ) : (一) Symptom severity scale (11 items)Document2 pagesBoston Carpal Tunnel Syndrome Questionnaire (BCTQ) : (一) Symptom severity scale (11 items)erlysaNo ratings yet
- Quick DASHDocument4 pagesQuick DASHKennedy Hindley100% (1)
- Quickda SH: Outcome MeasureDocument3 pagesQuickda SH: Outcome MeasureLuqmanul HakimNo ratings yet
- Lampiran Quick DASHDocument24 pagesLampiran Quick DASHhidayatul rahmo100% (1)
- DASH Questionnaire Disability Arm Shoulder HandDocument3 pagesDASH Questionnaire Disability Arm Shoulder HandChristopherLawrenceNo ratings yet
- New LongitudinalDocument2 pagesNew LongitudinalArijit DeyNo ratings yet
- Michigan Hand ScoreDocument6 pagesMichigan Hand ScoreRendy SusantoNo ratings yet
- SAQOL 39 Proxy Version Sr55z7Document5 pagesSAQOL 39 Proxy Version Sr55z7Fernanda VegaNo ratings yet
- UEFSDocument1 pageUEFSRiris WinchesterNo ratings yet
- Resource 365-1524656590442325921Document1 pageResource 365-1524656590442325921Danitza VeraNo ratings yet
- SAQOL 39 Self Complete 2exe584Document8 pagesSAQOL 39 Self Complete 2exe584paolo.nunzianteNo ratings yet
- QLQ-C30 English PDFDocument2 pagesQLQ-C30 English PDFabi nayaNo ratings yet
- Mathematics: Quarter 1 - Week 6 Lesson 1: Adding Fractions and Mixed NumbersDocument12 pagesMathematics: Quarter 1 - Week 6 Lesson 1: Adding Fractions and Mixed NumbersAmbass Ecoh67% (3)
- Lower Extremity Functional ScaleDocument3 pagesLower Extremity Functional Scalesonyanila0% (1)
- Brief Michigan Hand Questionnaire With ScoringDocument6 pagesBrief Michigan Hand Questionnaire With ScoringJavier Gomez LopezNo ratings yet
- Specimen Qlq-c30 EnglishDocument2 pagesSpecimen Qlq-c30 EnglishFenny KusumasariNo ratings yet
- Are Your ADLs Affected by HoardDocument2 pagesAre Your ADLs Affected by HoardKris LNo ratings yet
- Care and Comfort QuestionnaireDocument1 pageCare and Comfort Questionnairenavuru5kNo ratings yet
- Cuestionario FA12Document1 pageCuestionario FA12Julen Cruz QuiñonesNo ratings yet
- SF 36Document3 pagesSF 36Alessandro MedinaNo ratings yet
- SF 36Document3 pagesSF 36Ausias MuñozNo ratings yet
- Ullanlinna Narcolepsy ScaleDocument1 pageUllanlinna Narcolepsy Scalehcrislopes5617No ratings yet
- Sleep TestingDocument1 pageSleep TestingTroy O'BrienNo ratings yet
- Uefi 2010 PDFDocument1 pageUefi 2010 PDFRana M ArslanNo ratings yet
- WOMAC Knee Outcome MeasureDocument1 pageWOMAC Knee Outcome MeasuremitchNo ratings yet
- Escala PedsQL 5-7Document2 pagesEscala PedsQL 5-7Natalia GullónNo ratings yet
- FDI Child and ParentDocument2 pagesFDI Child and ParentOg DoogyNo ratings yet
- Zung Self-Rating Anxiety ScaleDocument2 pagesZung Self-Rating Anxiety Scale4perawatNo ratings yet
- WK 27-28 2019-20 2Document10 pagesWK 27-28 2019-20 2api-504873764No ratings yet
- ZA Zung Anxiety ScaleDocument1 pageZA Zung Anxiety ScaleKomala SariNo ratings yet
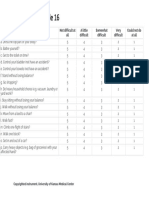
- Stroke Impact Scale 16Document1 pageStroke Impact Scale 16Cona KlaggesNo ratings yet
- Math - Gr6 - Q1 - Module 03-L2 - Problem-solving-Division-of-Fraction - PDF - 17pagesDocument18 pagesMath - Gr6 - Q1 - Module 03-L2 - Problem-solving-Division-of-Fraction - PDF - 17pagesOnin LampaNo ratings yet
- Career Assessment Battery - Oct. 2021 (1) EMMANUEL AFETIDocument3 pagesCareer Assessment Battery - Oct. 2021 (1) EMMANUEL AFETIEmmanuel AfetiNo ratings yet
- SDSC Eng ColourDocument2 pagesSDSC Eng ColourmerawatidyahsepitaNo ratings yet
- Nursing Outcomes Classification (NOC) : Popri Sri Istantiningsih, S.KepDocument27 pagesNursing Outcomes Classification (NOC) : Popri Sri Istantiningsih, S.Kepwawan kurniawanNo ratings yet
- Get Moving!: Solve Check and Look BackDocument1 pageGet Moving!: Solve Check and Look BackJoan Garay CarinanNo ratings yet
- HN43 EnglishDocument2 pagesHN43 EnglishAayush KapoorNo ratings yet
- Unit 2: Family Letter: Everyday Uses of NumbersDocument4 pagesUnit 2: Family Letter: Everyday Uses of NumbersAndrew FenstermakerNo ratings yet
- Stroke Impact Scale SISDocument6 pagesStroke Impact Scale SISJohann Sebastian CruzNo ratings yet
- Learning Objectives: Book 2 English For Professional NurseDocument3 pagesLearning Objectives: Book 2 English For Professional NurseFahmi SyarifNo ratings yet
- English - Yr 8 - Unit 2 - LA Task - Hatchet - ModifiedDocument5 pagesEnglish - Yr 8 - Unit 2 - LA Task - Hatchet - ModifiedBendigo South East CollegeNo ratings yet
- Zung Self-Rating Anxiety ScaleDocument1 pageZung Self-Rating Anxiety ScaleJoshuaSyaputraNo ratings yet
- Activity Sheet in Grade 5 Mathematics: I. Title: Division of FractionsDocument5 pagesActivity Sheet in Grade 5 Mathematics: I. Title: Division of FractionsShielo RestificarNo ratings yet
- Grade 9 - Unit 2 - WorkbookDocument28 pagesGrade 9 - Unit 2 - Workbookcutvanmai2903No ratings yet
- Lesson Plan in Mathematics IV RevisedDocument6 pagesLesson Plan in Mathematics IV RevisedNorol-in SabacanNo ratings yet
- Historical Development: Reported by Josephine P. Dela Vega Maed AlsDocument28 pagesHistorical Development: Reported by Josephine P. Dela Vega Maed AlsLevi BubanNo ratings yet
- Midterm Problem Set #2 AnswersDocument3 pagesMidterm Problem Set #2 AnswersJohn Arvin EscoteNo ratings yet
- Neck DisabilityDocument2 pagesNeck Disabilityjsyugesh21No ratings yet
- KN 459Document3 pagesKN 459Ret TrtNo ratings yet
- PrintDocument1 pagePrintjsyugesh21No ratings yet
- Ijms 24 04527 v2Document13 pagesIjms 24 04527 v2jsyugesh21No ratings yet
- Effect of Kinetic Chain Activation Technique in Shoulder Impairment: A ReviewDocument8 pagesEffect of Kinetic Chain Activation Technique in Shoulder Impairment: A Reviewjsyugesh21No ratings yet
- Updated Intake Packet 2020Document21 pagesUpdated Intake Packet 2020Allison GomoNo ratings yet
- Roy Adaptation ModelDocument2 pagesRoy Adaptation ModelYanny KimNo ratings yet
- Chapter 1 Class 11thDocument16 pagesChapter 1 Class 11thpsychshotsofficial2020No ratings yet
- Rational ChoiceDocument3 pagesRational ChoiceMonette M. VargasNo ratings yet
- DB Hse International PDF Notes - 3 PDFDocument21 pagesDB Hse International PDF Notes - 3 PDFKonan Jean Sylvère N'GORANNo ratings yet
- Annotated Bibliography-2Document4 pagesAnnotated Bibliography-2api-644291034No ratings yet
- Brittany Lozano HonorsThesisDocument147 pagesBrittany Lozano HonorsThesisKrisztian IndriesNo ratings yet
- Augmenting Roommate RelationshipDocument27 pagesAugmenting Roommate RelationshipAastha BhatraNo ratings yet
- Journal Entry #6. Worksheet On Developmental Tasks at HomeDocument2 pagesJournal Entry #6. Worksheet On Developmental Tasks at HomeWillian SeguerraNo ratings yet
- How To Attract Any Girl - The Art of CharmDocument9 pagesHow To Attract Any Girl - The Art of CharmZain Mra'i100% (1)
- Study Description RyanDocument2 pagesStudy Description RyanRyan ZhaoNo ratings yet
- Managing People and Organizations.: Assignment - Learning Outcome 01Document27 pagesManaging People and Organizations.: Assignment - Learning Outcome 01Namali De Silva0% (1)
- Religiosity and Death Anxiety Among Muslim Middle-Aged Adults in IndonesiaDocument7 pagesReligiosity and Death Anxiety Among Muslim Middle-Aged Adults in IndonesiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Grade 10 Thesis For ProcrastinationDocument10 pagesGrade 10 Thesis For ProcrastinationCabanizas DennielNo ratings yet
- Cultural Variations and Social Differences On Exceptionality/ Non-Exceptionality and NationalityDocument3 pagesCultural Variations and Social Differences On Exceptionality/ Non-Exceptionality and NationalitySagingNo ratings yet
- Attachment Dissertation TopicsDocument5 pagesAttachment Dissertation TopicsNeedHelpWritingAPaperWilmington100% (1)
- Circle of ControlDocument3 pagesCircle of ControlAlinedeOliveiraNo ratings yet
- Expert 6 - Review - Test - 5Document5 pagesExpert 6 - Review - Test - 5MarleneNo ratings yet
- Marriage Psychological Relationship," Love-ProblemDocument4 pagesMarriage Psychological Relationship," Love-ProblemMarko MlinaricNo ratings yet
- Chapter IiDocument9 pagesChapter IiMarco Miguel FranciaNo ratings yet
- Haddock & Maio 2017Document3 pagesHaddock & Maio 2017Diego ValenzuelaNo ratings yet
- AEGIS Candidate Application FormDocument9 pagesAEGIS Candidate Application FormKi NG HoNo ratings yet
- Interpersonal Skill AssessmentDocument6 pagesInterpersonal Skill AssessmentKaty DNo ratings yet
- Dokumen 2 ResumDocument14 pagesDokumen 2 ResumSiti BadariahNo ratings yet
- Lesson 3 Social WorkDocument1 pageLesson 3 Social WorkRushane MirandaNo ratings yet
- English 10 LAS Quarter 3 English 10 LAS Quarter 3Document45 pagesEnglish 10 LAS Quarter 3 English 10 LAS Quarter 3Kris Avein MalaayNo ratings yet
- Don't Watch The Clock Do What It Does. Keep Going!Document6 pagesDon't Watch The Clock Do What It Does. Keep Going!Sankale ShompoleNo ratings yet
- Care of ElderlyDocument23 pagesCare of Elderlyifer_018No ratings yet
- Workbook 4-5Document12 pagesWorkbook 4-5Fatima AlmohannadiNo ratings yet
- 1.research DesignDocument14 pages1.research DesignJhamille CardonaNo ratings yet