Name ____________________________________ Date ________________ Patient ID#_______________
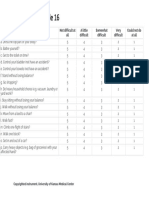
Lower Extremity Functional Scale
We are interested in knowing whether you are having any difficulty with the activities listed below
because of your lower limb problem for which you are currently seeking attention. Provide an answer
for each activity.
Today, do you or would you have any difficulty with: (Circle one number on each line)
Extreme
Difficulty Quite a A Little
or Unable Bit of Moderate Bit of No
to Perform Difficulty Difficulty Difficulty Difficulty
Activities Activity
a. Any of your usual work, household, or 0 1 2 3 4
school activities.
b. Your usual hobbies, recreational or 0 1 2 3 4
sporting activities.
c. Getting into or out of the bath. 0 1 2 3 4
d. Walking between rooms. 0 1 2 3 4
e. Putting on your shoes or socks. 0 1 2 3 4
f. Squatting. 0 1 2 3 4
g. Lifting an object, like a bag of groceries 0 1 2 3 4
from the floor.
h. Performing light activities around your 0 1 2 3 4
home.
i. Performing heavy activities around your 0 1 2 3 4
home.
j. Getting into or out of a car. 0 1 2 3 4
k. Walking 2 blocks. 0 1 2 3 4
l. Walking a mile. 0 1 2 3 4
m. Going up or down 10 stairs (about 1 flight 0 1 2 3 4
of stairs).
n. Standing for 1 hour. 0 1 2 3 4
o. Sitting for 1 hour. 0 1 2 3 4
p. Running on even ground. 0 1 2 3 4
q. Running on uneven ground 0 1 2 3 4
r. Making sharp turns while running fast 0 1 2 3 4
s. Hopping 0 1 2 3 4
t. Rolling over in bed 0 1 2 3 4
COLUMN TOTALS (for physical therapist use)
Score is the sum of all circled items. (range = 0-80) Score: _/80
You might also like
- Wordly Wise Book2Document153 pagesWordly Wise Book2Via Rabe100% (24)
- SLEEP HYGIENE INDEX DrWendieRobbins PDFDocument1 pageSLEEP HYGIENE INDEX DrWendieRobbins PDFrinaldy andriansyahNo ratings yet
- SLEEP HYGIENE INDEX DrWendieRobbins PDFDocument1 pageSLEEP HYGIENE INDEX DrWendieRobbins PDFrinaldy andriansyahNo ratings yet
- SLEEP HYGIENE INDEX DrWendieRobbins PDFDocument1 pageSLEEP HYGIENE INDEX DrWendieRobbins PDFrinaldy andriansyahNo ratings yet
- DashDocument1 pageDashKathryn LasNo ratings yet
- Foot Function IndexDocument1 pageFoot Function IndexVALENNo ratings yet
- Steven Connor, Postmodernist CultureDocument366 pagesSteven Connor, Postmodernist CultureME50% (2)
- WOMAC Knee Outcome MeasureDocument1 pageWOMAC Knee Outcome MeasuremitchNo ratings yet
- Escala PedsQL 5-7Document2 pagesEscala PedsQL 5-7Natalia GullónNo ratings yet
- User Manual MotorsDocument31 pagesUser Manual MotorsCosmin CabaroiuNo ratings yet
- UEFSDocument1 pageUEFSRiris WinchesterNo ratings yet
- LEFSDocument1 pageLEFSMorteza BahramiNo ratings yet
- Uefi 2010 PDFDocument1 pageUefi 2010 PDFRana M ArslanNo ratings yet
- Lefs PDFDocument1 pageLefs PDFAbbyGael Fikri MNo ratings yet
- Lefs CleanDocument1 pageLefs CleanMarlou II PonteNo ratings yet
- Lower Extremity Functional ScaleDocument3 pagesLower Extremity Functional Scalesonyanila0% (1)
- The Western Ontario and Mcmaster Universities Osteoarthritis Index (Womac)Document1 pageThe Western Ontario and Mcmaster Universities Osteoarthritis Index (Womac)Carlos Daniel da Silva AlonsoNo ratings yet
- FDI Child and ParentDocument2 pagesFDI Child and ParentOg DoogyNo ratings yet
- The Quebec Back Pain Disability ScaleDocument2 pagesThe Quebec Back Pain Disability ScaleFranci SzaboNo ratings yet
- DR Tuna Dash FormDocument5 pagesDR Tuna Dash Formjsyugesh21No ratings yet
- Upper Extremity PDFDocument1 pageUpper Extremity PDFShinta S. AnzaniNo ratings yet
- The Upper Extremity Functional Index (Uefi) : Today, Do You or Would You Have Any Difficulty at All WithDocument1 pageThe Upper Extremity Functional Index (Uefi) : Today, Do You or Would You Have Any Difficulty at All WithYashaswi ANo ratings yet
- Upper ExtremityDocument1 pageUpper ExtremityJesse ManekNo ratings yet
- Upper Extremity PDFDocument1 pageUpper Extremity PDFShinta S. AnzaniNo ratings yet
- Upper Extremity PDFDocument1 pageUpper Extremity PDFShinta S. AnzaniNo ratings yet
- DASHDocument2 pagesDASHNICOLE RAFAEL TACDERASNo ratings yet
- DashDocument4 pagesDashjsyugesh21No ratings yet
- NAME: Alex N. Manalo Section: Modesty: Week 3/ Lesson 3Document6 pagesNAME: Alex N. Manalo Section: Modesty: Week 3/ Lesson 3Zameer Drake NuiqueNo ratings yet
- Carpal Tunnel Syndrome Questionnaire (CTSQ)Document1 pageCarpal Tunnel Syndrome Questionnaire (CTSQ)Samuel Iñiguez JiménezNo ratings yet
- Foot Ankle Ability Measure FaamDocument3 pagesFoot Ankle Ability Measure FaamGeetha BalasubramanianNo ratings yet
- Cyrus Agconol DemoDocument4 pagesCyrus Agconol DemoCYRUS ANDREA AGCONOLNo ratings yet
- Direct Variation I. ObjectivesDocument9 pagesDirect Variation I. ObjectivesRomalyn VillegasNo ratings yet
- 1 Instrumen QOL General Usia 2 Sampai 4 TahunDocument2 pages1 Instrumen QOL General Usia 2 Sampai 4 TahunmuarifNo ratings yet
- Stroke Impact Scale 16Document1 pageStroke Impact Scale 16Cona KlaggesNo ratings yet
- International Knee Documentation Committee Subjective Knee Evaluation FormDocument5 pagesInternational Knee Documentation Committee Subjective Knee Evaluation FormNabilNo ratings yet
- TWSTRSDocument1 pageTWSTRSfirmandotindraNo ratings yet
- Artificial IntelligenceDocument106 pagesArtificial IntelligenceCharith RcNo ratings yet
- FES-I EnglishDocument1 pageFES-I EnglishMochammad Syarif Hidayat100% (1)
- Anxiety Scale: Dr. Reneé Roberts, PsychologistDocument3 pagesAnxiety Scale: Dr. Reneé Roberts, Psychologistpreeti vermaNo ratings yet
- Year 4 Spelling ListDocument4 pagesYear 4 Spelling ListaguliewNo ratings yet
- woodlice范文Document6 pageswoodlice范文Zia Baerfuss-liaoNo ratings yet
- 4 Semana 15Document20 pages4 Semana 15Estela VivianaNo ratings yet
- Extra Vocabulary: Extension Units 1 & 2Document1 pageExtra Vocabulary: Extension Units 1 & 2Wayra BANo ratings yet
- Plan Lector - 4to Grado - DMpA 14 - Unit 4Document3 pagesPlan Lector - 4to Grado - DMpA 14 - Unit 4JAIR JERSON VILLENA TORRESNo ratings yet
- Wolf Motor Function Test WMFTDocument1 pageWolf Motor Function Test WMFTTadeja Hernja Rumpf100% (1)
- Solving Rubik's Cube: Solving The Upper LayerDocument9 pagesSolving Rubik's Cube: Solving The Upper Layerben_c_noel93No ratings yet
- Sleep InterviewDocument4 pagesSleep InterviewFatemah BeygNo ratings yet
- Learning Activity Sheet in ScienceDocument10 pagesLearning Activity Sheet in Sciencesandra bumalayNo ratings yet
- 1 Instrumen QOL General Usia 2 Sampai 4 TahunDocument2 pages1 Instrumen QOL General Usia 2 Sampai 4 TahunmuarifNo ratings yet
- SAQOL 39 Self Complete 2exe584Document8 pagesSAQOL 39 Self Complete 2exe584paolo.nunzianteNo ratings yet
- Boston Carpal Tunnel Questionnaire BCTSQDocument2 pagesBoston Carpal Tunnel Questionnaire BCTSQmario benjamin suarez carcamoNo ratings yet
- Care and Comfort QuestionnaireDocument1 pageCare and Comfort Questionnairenavuru5kNo ratings yet
- Peds QL 13-18 THDocument2 pagesPeds QL 13-18 THAndra KurniantoNo ratings yet
- HW# (1,2)Document8 pagesHW# (1,2)Bashir AlsadawiNo ratings yet
- A Detailed Lesson Plan in T.L.E Grade VI I. Objectives: by Erica Oblepias CalcetasDocument6 pagesA Detailed Lesson Plan in T.L.E Grade VI I. Objectives: by Erica Oblepias CalcetasMarvinNo ratings yet
- Work Calculation ProblemDocument2 pagesWork Calculation ProblemBhubha KasikidnumchaiNo ratings yet
- 05 Sequence AdverbsDocument1 page05 Sequence Adverbshakerwey hakerweyNo ratings yet
- Nguyễn Thu Thảo - 10E1 - Unit 7 - Lesson 11.3 - Nature's forcesDocument20 pagesNguyễn Thu Thảo - 10E1 - Unit 7 - Lesson 11.3 - Nature's forcesNguyễn Thị NgọcNo ratings yet
- Math 4Document9 pagesMath 4Jonabelle BalasabasNo ratings yet
- With Rcgud Written Usig - Nmenu. Cxhof Following: How Skill JS, A..ndDocument1 pageWith Rcgud Written Usig - Nmenu. Cxhof Following: How Skill JS, A..ndfalih arshiya12No ratings yet
- Best PC Cheats for Miners: (An Unofficial Minecraft Book)From EverandBest PC Cheats for Miners: (An Unofficial Minecraft Book)No ratings yet
- Paints and CoatingsDocument29 pagesPaints and CoatingsRai JeanNo ratings yet
- Percy Jackson MovieDocument1 pagePercy Jackson MovieRegie Rey Agustin100% (1)
- Auditorium SH1 PDFDocument1 pageAuditorium SH1 PDFPRATIMA MAHADIKNo ratings yet
- Caroline Odwyer ResumeDocument1 pageCaroline Odwyer Resumeapi-141027160No ratings yet
- The Use of The Past in Denis Scott An EcHO IN THE BONEDocument2 pagesThe Use of The Past in Denis Scott An EcHO IN THE BONEKaycia HyltonNo ratings yet
- Pfof1950 V01 PDFDocument1,006 pagesPfof1950 V01 PDFFilep-LukácsIstvánNo ratings yet
- HoA 2 ReviewerDocument9 pagesHoA 2 ReviewerSamänthä Mae ParladeNo ratings yet
- Cambridge Secondary 1 CheckpointDocument12 pagesCambridge Secondary 1 CheckpointAizat Zulhilmi YusupNo ratings yet
- 8th Grade Summer Review Quiz (Grade 8) - Free Printable Tests and Worksheets PDFDocument4 pages8th Grade Summer Review Quiz (Grade 8) - Free Printable Tests and Worksheets PDFLerato TlakaneNo ratings yet
- Promise Kept For John Anderson's Biggest Fan, His DaughterDocument3 pagesPromise Kept For John Anderson's Biggest Fan, His DaughterDaniel HouseNo ratings yet
- What Shall We Do With The Drunken SailorDocument24 pagesWhat Shall We Do With The Drunken SailorMike HatchardNo ratings yet
- Micah Myers - Comic Book Lettering PortfolioDocument25 pagesMicah Myers - Comic Book Lettering PortfolioMicah MyersNo ratings yet
- MHAWK LHD Manual Electrico PDFDocument52 pagesMHAWK LHD Manual Electrico PDFAlex BravoNo ratings yet
- Manuscript Releases Vol 3Document254 pagesManuscript Releases Vol 3chechi10No ratings yet
- Spirit: Stallion of The CimmaronDocument5 pagesSpirit: Stallion of The CimmaronShashwata DattaNo ratings yet
- Khalil GibranDocument2 pagesKhalil GibranLutfiArdiningTyasNo ratings yet
- PDF To Autocad - Google SearchDocument3 pagesPDF To Autocad - Google SearchMuhafeez GoolabNo ratings yet
- Mundo ChordsDocument10 pagesMundo Chordsangel100% (1)
- Bajou CV 2019 PDFDocument14 pagesBajou CV 2019 PDFEstelle BajouNo ratings yet
- Adjust Global App Trends 2019Document35 pagesAdjust Global App Trends 2019MetropolesNo ratings yet
- An Analysis of Stephen Dedalus in A Portrait of The Artist As A YoungDocument4 pagesAn Analysis of Stephen Dedalus in A Portrait of The Artist As A YoungSeabiscuit NygmaNo ratings yet
- Brad Farrell - RésuméDocument1 pageBrad Farrell - RésuméBrad FarrellNo ratings yet
- Himachal Report A3 Low LowDocument43 pagesHimachal Report A3 Low Lowapi-241074820No ratings yet
- New Light Green Energy LED PDFDocument40 pagesNew Light Green Energy LED PDFDeny AlfonsoNo ratings yet
- ... Radial DraperyDocument4 pages... Radial DraperyAmandaNo ratings yet
- July 2010 Uptown Neighborhood NewsDocument12 pagesJuly 2010 Uptown Neighborhood NewsUptownNewsNo ratings yet
- FormDocument2 pagesFormKamrankhan KamranNo ratings yet
- MC Script 4 RecogDocument2 pagesMC Script 4 RecogArjel DantesNo ratings yet