You might also like
- Step 2 CK Usmle Questions For Ob GynDocument48 pagesStep 2 CK Usmle Questions For Ob Gyniamdonut87% (15)
- Tamil Siddhar Jeeva Samadhi PDFDocument23 pagesTamil Siddhar Jeeva Samadhi PDFsenthilkumar100% (1)
- Obstetric ExamDocument35 pagesObstetric ExamRafi MahandaruNo ratings yet
- Soal Unas Maret 2016 - Agustus 2020Document274 pagesSoal Unas Maret 2016 - Agustus 2020Hambrian WijayaNo ratings yet
- Blueprints Obstetrics and Gynecology 5th Edition MCQDocument30 pagesBlueprints Obstetrics and Gynecology 5th Edition MCQsinglez100% (1)
- Fritz Springmeier InterviewDocument59 pagesFritz Springmeier InterviewCzink Tiberiu100% (4)
- USULDocument6 pagesUSULdika putrayudaNo ratings yet
- Questions 5 To 8Document26 pagesQuestions 5 To 8Stefannus Wibisono100% (1)
- Dokterpost - 24 - 26122022Document97 pagesDokterpost - 24 - 26122022Prima DianaNo ratings yet
- AttachmentDocument10 pagesAttachmentdheasuyuthiNo ratings yet
- Juli 2018Document31 pagesJuli 2018Chynthea ParamithaNo ratings yet
- Unas Mei 2020 (Sule) : Yang Dianggap Soal BaruDocument15 pagesUnas Mei 2020 (Sule) : Yang Dianggap Soal Baruhari ilman toniNo ratings yet
- Soal Usulan Unas Unhas November 2018Document26 pagesSoal Usulan Unas Unhas November 2018Umaimah ShahabNo ratings yet
- Unas Maret 2018Document32 pagesUnas Maret 2018Dewi Arianti BudiantoNo ratings yet
- Obs 7th Sem Mid TermDocument5 pagesObs 7th Sem Mid Termaparna shama100% (1)
- Juli 2022Document28 pagesJuli 2022Chynthea ParamithaNo ratings yet
- Exam Sample:: B. Cervical Incompetence and Cervical StenosisDocument3 pagesExam Sample:: B. Cervical Incompetence and Cervical StenosisSiraj Ul IslamNo ratings yet
- Tes 1Document6 pagesTes 1dika putrayudaNo ratings yet
- Obstetrics MukundaDocument48 pagesObstetrics Mukundadocivirus100% (1)
- Agustus 2020Document24 pagesAgustus 2020Chynthea ParamithaNo ratings yet
- AntePartum Hemorrhage (Blueprints 2017)Document20 pagesAntePartum Hemorrhage (Blueprints 2017)Mandala putra IlhamNo ratings yet
- DR Nadine Rev All (Samra's Edition)Document313 pagesDR Nadine Rev All (Samra's Edition)Cyril I.Makar100% (1)
- E. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborDocument10 pagesE. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborSK ASIF ALINo ratings yet
- OB-GYNE 2 Batch 2017 Ratio PDFDocument13 pagesOB-GYNE 2 Batch 2017 Ratio PDFAdrianNo ratings yet
- WHISM WH MCQ Paper 2020Document22 pagesWHISM WH MCQ Paper 2020hexagridledsNo ratings yet
- MCQ Remake Group A 2022Document16 pagesMCQ Remake Group A 2022V Sugrim100% (1)
- OA 6 SeptDocument19 pagesOA 6 Septstella pangestikaNo ratings yet
- Tes PanoramaDocument57 pagesTes Panoramamuttaqin95No ratings yet
- UNAS 59th (NOV 2020) FIXDocument23 pagesUNAS 59th (NOV 2020) FIXmhariskurniawanNo ratings yet
- Soal Usulan UnHas Juli 2019Document25 pagesSoal Usulan UnHas Juli 2019Ibnu SinaNo ratings yet
- Multiple ChoiceDocument55 pagesMultiple Choicetri ebtaNo ratings yet
- Obs 1 Bleeding in Early Pregnancy QuestionsDocument9 pagesObs 1 Bleeding in Early Pregnancy QuestionsSalmonella TyphiNo ratings yet
- 3 16Document27 pages3 16Iful SaifullahNo ratings yet
- Reproductive (Female)Document15 pagesReproductive (Female)Vinnydapooh BearNo ratings yet
- Ats Menjawab Super Brankas Soal Unas 2020-2015Document424 pagesAts Menjawab Super Brankas Soal Unas 2020-2015anton suponoNo ratings yet
- Recall January 2018-2Document38 pagesRecall January 2018-2Umme Habiba GilaniNo ratings yet
- Ats Menjawab Soal Unas November 2021 EditedDocument26 pagesAts Menjawab Soal Unas November 2021 Editedanton suponoNo ratings yet
- Ginek DasarDocument18 pagesGinek DasarEduward PasangkaNo ratings yet
- Obstetrics and Gynecology》考试试卷 (A) : Name Class FacultyDocument7 pagesObstetrics and Gynecology》考试试卷 (A) : Name Class FacultyNidya PutrijNo ratings yet
- MCQ 22 PDFDocument7 pagesMCQ 22 PDFirynNo ratings yet
- Obs MCQDocument13 pagesObs MCQaaycee100% (3)
- 46 60Document7 pages46 60member12dNo ratings yet
- Lengkap 1Document38 pagesLengkap 1Stefannus WibisonoNo ratings yet
- UNAS Nov 2019Document25 pagesUNAS Nov 2019paramitastellaNo ratings yet
- A 18-Year-Old G1 at 30 4/7 Weeks Presents For Her Scheduled Obstet Ric (OB) Appointment. A 28-Week Ultrasound Showed The Fetus To BDocument13 pagesA 18-Year-Old G1 at 30 4/7 Weeks Presents For Her Scheduled Obstet Ric (OB) Appointment. A 28-Week Ultrasound Showed The Fetus To BHambrian WijayaNo ratings yet
- Unas Agustus 2017Document18 pagesUnas Agustus 2017Dewi Arianti BudiantoNo ratings yet
- Obstetrics and Gyn Outline - NBMEDocument6 pagesObstetrics and Gyn Outline - NBMEGameron777No ratings yet
- Soal Ujian R2 FixedDocument9 pagesSoal Ujian R2 Fixedprakoso jatiNo ratings yet
- University of Santo TomasDocument28 pagesUniversity of Santo TomasLyndon SayongNo ratings yet
- The Test May Be Run On Patients Between 22 and 34 Weeks GestationDocument6 pagesThe Test May Be Run On Patients Between 22 and 34 Weeks Gestationdaniel_alexander_susenoNo ratings yet
- EMQ Paper1with Answers Jan 2012Document9 pagesEMQ Paper1with Answers Jan 2012Hasan DahamshehNo ratings yet
- Whism WH MCQ Paper 2019Document12 pagesWhism WH MCQ Paper 2019hexagridledsNo ratings yet
- LATIHAN TIM SUKSES Unas (Autosaved)Document52 pagesLATIHAN TIM SUKSES Unas (Autosaved)yoga paripurnaNo ratings yet
- ATS Menjawab Soal UKN Maret 2021 HQQDocument18 pagesATS Menjawab Soal UKN Maret 2021 HQQanton suponoNo ratings yet
- 1519 - 109 - 1 - Case Studies in Reproductive Endocrinology InfertiDocument33 pages1519 - 109 - 1 - Case Studies in Reproductive Endocrinology InfertiWael GaberNo ratings yet
- 2022-23 OBG MMed 2 - 3btest 1 - KeyDocument12 pages2022-23 OBG MMed 2 - 3btest 1 - KeyKenneth ChandaNo ratings yet
- Gynae-L - MukundaDocument50 pagesGynae-L - MukundadocivirusNo ratings yet
- Whism WH 2021 MCQ PaperDocument15 pagesWhism WH 2021 MCQ PaperhexagridledsNo ratings yet
- ملزمة القبالة-dddd4Document120 pagesملزمة القبالة-dddd4Shama Awwad100% (1)
- Mcqs - Obstetrics and Gynaecology (For Post Graduate Preparing For FNB and Professionals) Obstetrics and GynaecologyDocument27 pagesMcqs - Obstetrics and Gynaecology (For Post Graduate Preparing For FNB and Professionals) Obstetrics and GynaecologyAnonymous kQCQ30Rq5ONo ratings yet
- Medical School Companion Obstetrics and Gynecology Practice Question BookFrom EverandMedical School Companion Obstetrics and Gynecology Practice Question BookNo ratings yet
- Unit 13. Tidy Up!Document10 pagesUnit 13. Tidy Up!Nguyễn Thị Ngọc HuyềnNo ratings yet
- The Rook Volume XXIIIDocument40 pagesThe Rook Volume XXIIIThe RookNo ratings yet
- Arts - 9 - Quarter 3 Module 1Document4 pagesArts - 9 - Quarter 3 Module 1John Mark Prestoza100% (3)
- 2006 Amc8Document12 pages2006 Amc8Yuhang HeNo ratings yet
- B2 Unit 4 Reading Plus LessonDocument2 pagesB2 Unit 4 Reading Plus LessonIruneNo ratings yet
- Long Quiz 1 Eim Tools, MaterialsDocument1 pageLong Quiz 1 Eim Tools, MaterialsLea Ann PalaciosNo ratings yet
- Kerala University PHD Course Work Exam SyllabusDocument4 pagesKerala University PHD Course Work Exam Syllabuslozuzimobow3100% (2)
- WWII Europe Organization ChartsDocument56 pagesWWII Europe Organization ChartsCAP History Library100% (1)
- SaviorKitty - (Seven Deadly Sins Series 4) PrideDocument48 pagesSaviorKitty - (Seven Deadly Sins Series 4) PrideMarife LuzonNo ratings yet
- ED 305 Calvin College Lesson Planning FormDocument4 pagesED 305 Calvin College Lesson Planning Formapi-314250067No ratings yet
- New Microsoft Word DocumentDocument2 pagesNew Microsoft Word Documenthakimfriends3No ratings yet
- From St. Francis To Dante-Translations From The Chronicle of The Franciscan Salimbene, 1221-1288Document489 pagesFrom St. Francis To Dante-Translations From The Chronicle of The Franciscan Salimbene, 1221-1288Jake SalNo ratings yet
- Electric Charges & Fields: Chapter-1 class-XIIDocument20 pagesElectric Charges & Fields: Chapter-1 class-XIIMohit SahuNo ratings yet
- Timeline of My Exposure To Traditional and New Media - Justine Sheen Gay-12 ABM-BDocument16 pagesTimeline of My Exposure To Traditional and New Media - Justine Sheen Gay-12 ABM-Bapi-389627320No ratings yet
- History of Madre de DiosDocument3 pagesHistory of Madre de DiosMisterJanNo ratings yet
- Writing Task 2 - Discussion - Opinion EssayDocument7 pagesWriting Task 2 - Discussion - Opinion EssayTonNo ratings yet
- WN Ce1905 enDocument3 pagesWN Ce1905 enanuagarwal anuNo ratings yet
- Say's Law of Market and Quantity Theory of MoneyDocument19 pagesSay's Law of Market and Quantity Theory of MoneyBHANU TYAGINo ratings yet
- Solar Geometry FinalDocument17 pagesSolar Geometry Finalsarvesh kumarNo ratings yet
- Your Best American GirlDocument9 pagesYour Best American GirlCrystaelechanNo ratings yet
- CH 1 Cases - Mcqs CH 1 Cases - McqsDocument55 pagesCH 1 Cases - Mcqs CH 1 Cases - McqsChaudhary AdeelNo ratings yet
- SnapManual PDFDocument77 pagesSnapManual PDFnaser150No ratings yet
- Containers For Every Need: Maersk Equipment GuideDocument12 pagesContainers For Every Need: Maersk Equipment GuideSharath RadhakrishnanNo ratings yet
- Fforde Economic StrategyDocument29 pagesFforde Economic StrategyDinhThuyNo ratings yet
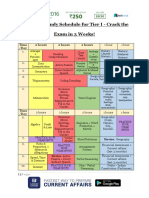
- SSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Document3 pagesSSC CHSL Study Schedule For Tier I - Crack The Exam in 3 Weeks!Tushita80% (15)
- Ec04c0a5 en GBDocument3 pagesEc04c0a5 en GBd228835No ratings yet
- Gian Jyoti Institute of Management and Technology, Mohali Assignment No-1 Academic Session January-May 202Document4 pagesGian Jyoti Institute of Management and Technology, Mohali Assignment No-1 Academic Session January-May 202Isha aggarwalNo ratings yet
- Music For BandDocument143 pagesMusic For BandTedTerroux604No ratings yet