You might also like
- Case Study On Pre EclampsiaDocument21 pagesCase Study On Pre EclampsiaKavi rajput95% (21)
- Shubham Singh Thesis ReportDocument52 pagesShubham Singh Thesis ReportShubham Singh71% (7)
- Case Study On Uterine ProlapseDocument17 pagesCase Study On Uterine Prolapsepriyanka100% (7)
- Case Presentation On AphDocument20 pagesCase Presentation On AphDeepti Kukreti86% (14)
- CaseDocument54 pagesCaseRaja100% (4)
- The Ayurvedic Reset Diet: Radiant Health through Fasting, Mono-Diet, and Smart Food CombiningFrom EverandThe Ayurvedic Reset Diet: Radiant Health through Fasting, Mono-Diet, and Smart Food CombiningRating: 2 out of 5 stars2/5 (1)
- Case Study of Placenta PreviaDocument24 pagesCase Study of Placenta Previajeelani saima86% (37)
- Case Study FinalDocument31 pagesCase Study FinalRajaNo ratings yet
- CP PihDocument33 pagesCP PihArchita SharmaNo ratings yet
- Bicornuate Unicolli Uterus 2Document46 pagesBicornuate Unicolli Uterus 2Anjali LimbuNo ratings yet
- Nephrotic SyndromeDocument38 pagesNephrotic SyndromeSwati SharmaNo ratings yet
- Case Presentation On AphDocument20 pagesCase Presentation On AphAnkita SamantaNo ratings yet
- Case Presentation ON Puerperial Sepsis: Submitted ToDocument12 pagesCase Presentation ON Puerperial Sepsis: Submitted ToPriyanka John100% (1)
- Case Study Placenta PreviaDocument26 pagesCase Study Placenta PreviaSusmita SenNo ratings yet
- INTUSSUSCEPTIONDocument43 pagesINTUSSUSCEPTIONValarmathi100% (3)
- Labor Room (Intranatal Care Plan)Document11 pagesLabor Room (Intranatal Care Plan)Bhumi ChouhanNo ratings yet
- Case Study On Ca GallbladderDocument45 pagesCase Study On Ca GallbladderKhushboo KerkettaNo ratings yet
- Care Plan BRAIN TUMORDocument16 pagesCare Plan BRAIN TUMORELISION OFFICIALNo ratings yet
- AnemiaDocument40 pagesAnemiaRajaNo ratings yet
- Pulmonary EdemaDocument23 pagesPulmonary EdemaELISION OFFICIALNo ratings yet
- Vomiting in PregnancyDocument13 pagesVomiting in PregnancyPriyanka John100% (4)
- Nutritional AsthaDocument30 pagesNutritional AsthaSwati SharmaNo ratings yet
- Amity College of Nursing: Nursing Care Plan ON Heart FailureDocument20 pagesAmity College of Nursing: Nursing Care Plan ON Heart Failurejyoti punia100% (1)
- Care Plan AnaemiaDocument16 pagesCare Plan AnaemiaSusmita SenNo ratings yet
- P SepsisDocument11 pagesP SepsisDaily DoseNo ratings yet
- Case Report Session Bronkopneumonia: Disusun Oleh: Dr. Cindy Amalia Dokter Pendamping: Dr. Hj. SumarmiDocument30 pagesCase Report Session Bronkopneumonia: Disusun Oleh: Dr. Cindy Amalia Dokter Pendamping: Dr. Hj. Sumarmidenokkosasi100% (1)
- CP 1Document18 pagesCP 1Rubina MasihNo ratings yet
- Case Presentation On DepressionDocument22 pagesCase Presentation On DepressionSakshi AsthanaNo ratings yet
- Case ReportDocument24 pagesCase ReportSyifar100% (1)
- Health Assessment Peptic UlcerDocument13 pagesHealth Assessment Peptic UlcerHimani PatelNo ratings yet
- Pediatic Case Presentation FinalDocument26 pagesPediatic Case Presentation FinalJyoti Prem UttamNo ratings yet
- Obg - Case Presentation - FGRDocument24 pagesObg - Case Presentation - FGRNazee NazreenNo ratings yet
- NCP PostnatalDocument37 pagesNCP PostnatalNadiya Rashid86% (7)
- PNC PresentationDocument42 pagesPNC PresentationRijoy ZuzadNo ratings yet
- Cwu O&g 1 PPROMDocument13 pagesCwu O&g 1 PPROMFaris Mohd Nasir100% (1)
- Preterm Breech Case StudyDocument10 pagesPreterm Breech Case StudyYa Mei LiNo ratings yet
- Case Study On Cerebral PalsyDocument37 pagesCase Study On Cerebral PalsyISLAMIC KNOWLEDGE BASED ON TRULY HADIS60% (5)
- Case Presentation On TuberculosisDocument36 pagesCase Presentation On TuberculosisLavie Gangwar100% (2)
- VacuumDocument22 pagesVacuumRed WilliamsNo ratings yet
- Gyne Case PresentationDocument12 pagesGyne Case PresentationTada MinionNo ratings yet
- ANC CaseDocument21 pagesANC CaseShaliniNo ratings yet
- Pcos Case StudyDocument33 pagesPcos Case StudyAli AkbarNo ratings yet
- Twin PregnancyDocument23 pagesTwin PregnancyNazee NazreenNo ratings yet
- Breech Case StudyDocument31 pagesBreech Case StudyJones KondoweNo ratings yet
- @ - Seminar KariadiDocument14 pages@ - Seminar KariadiAgus Dwi SiswantoNo ratings yet
- 1696-Article Text-4009-1-10-20201129Document5 pages1696-Article Text-4009-1-10-20201129asmita sainiNo ratings yet
- CASE STUDY (ABNORMAL PREGNANCY) .Edited (2)Document9 pagesCASE STUDY (ABNORMAL PREGNANCY) .Edited (2)niyoc68859No ratings yet
- 3 Care PlanDocument25 pages3 Care PlanKhushbu KatariaNo ratings yet
- Case Study On RDSDocument43 pagesCase Study On RDSNeha Patel100% (1)
- Case Study On IBDDocument41 pagesCase Study On IBDchampaNo ratings yet
- ASUHAN KEBIDANAN KEHAMILAN PKKBDocument12 pagesASUHAN KEBIDANAN KEHAMILAN PKKBInggrit Novisari RatuNo ratings yet
- CP Acute and Chornic DiseaseDocument27 pagesCP Acute and Chornic DiseaseTopeshwar TpkNo ratings yet
- Case Study On Wilson's DiseaseDocument49 pagesCase Study On Wilson's Diseaseamit100% (1)
- Care Plan On: Submitted To: Submitted byDocument38 pagesCare Plan On: Submitted To: Submitted byMoonNo ratings yet
- Case Presentation On GbsDocument23 pagesCase Presentation On GbsRucHi ShArmaNo ratings yet
- Case Study of Placenta PreviaDocument23 pagesCase Study of Placenta PreviaPreeti ChouhanNo ratings yet
- Clinical Presentation On ObgDocument20 pagesClinical Presentation On ObgValarmathiNo ratings yet
- Report of Care Plan On Op Poisoining': Tribhuvan UniversityDocument12 pagesReport of Care Plan On Op Poisoining': Tribhuvan UniversitySushmaNo ratings yet
- Case Study - NSVDDocument47 pagesCase Study - NSVDJoyJoy Tabada CalunsagNo ratings yet
- Nursing Process Antental1Document11 pagesNursing Process Antental1MANOJNo ratings yet
- Your Vegetarian Pregnancy: A Month-by-Month Guide to Health and NutritionFrom EverandYour Vegetarian Pregnancy: A Month-by-Month Guide to Health and NutritionRating: 5 out of 5 stars5/5 (4)
- Case Study ITPDocument45 pagesCase Study ITPberty dennyNo ratings yet
- Achondroplasia in A Children With VentriculomegalyDocument70 pagesAchondroplasia in A Children With Ventriculomegalydr_aldilapratiwiNo ratings yet
- Programme 63rd Annual Conference of WACS, Lome, TogoDocument51 pagesProgramme 63rd Annual Conference of WACS, Lome, TogoAchille DoleagbenouNo ratings yet
- UWSA1 - ReviewDocument160 pagesUWSA1 - ReviewrabieeNo ratings yet
- Health Schemes and Yojana IndiaDocument4 pagesHealth Schemes and Yojana IndiaKailash Nagar100% (1)
- Thesis About Early Pregnancy in The PhilippinesDocument5 pagesThesis About Early Pregnancy in The Philippinesdarlenetourignysaltlakecity100% (2)
- Hypertension in PregnancyDocument18 pagesHypertension in Pregnancyshubham kumarNo ratings yet
- Mother&child - Rights - Immigrants in NorwayDocument86 pagesMother&child - Rights - Immigrants in NorwayAy GunNo ratings yet
- Community WrittenDocument23 pagesCommunity WrittenImPrint CenterNo ratings yet
- Osce: Outlet Forceps ExtractionDocument2 pagesOsce: Outlet Forceps ExtractionValerie Gonzaga-CarandangNo ratings yet
- Antenatal Steroids - Role in NeonatologyDocument62 pagesAntenatal Steroids - Role in NeonatologyRadhika BatraNo ratings yet
- Handbook Obs & GynDocument48 pagesHandbook Obs & GyndoodrillNo ratings yet
- Ovarian TorsionDocument48 pagesOvarian Torsionmaria ilyasNo ratings yet
- HypersensitivityDocument27 pagesHypersensitivityboscomooliNo ratings yet
- Asuhan Kebidanan Nifas Dan Menyusui (Juli Claudia) PDFDocument621 pagesAsuhan Kebidanan Nifas Dan Menyusui (Juli Claudia) PDFPutry UtinaNo ratings yet
- Information For You: Pelvic Organ ProlapseDocument8 pagesInformation For You: Pelvic Organ Prolapsesandeepv08No ratings yet
- G8-Health-Q2-LM-Family Health IIDocument61 pagesG8-Health-Q2-LM-Family Health IIEvangeline A. AlegreNo ratings yet
- CH 47 - Animal DevelopmentDocument70 pagesCH 47 - Animal DevelopmentSofiaNo ratings yet
- Complications During Pregnancy 1Document5 pagesComplications During Pregnancy 1Ace Brian BaraoidanNo ratings yet
- Patient Assessment A. HistoryDocument32 pagesPatient Assessment A. HistoryTHE HOWDAY COMPANYNo ratings yet
- MCN-RLE - Quiz#1. Ramos, L.Document3 pagesMCN-RLE - Quiz#1. Ramos, L.Louwella RamosNo ratings yet
- Menorrhagia (Heavy Menstrual Bleeding)Document55 pagesMenorrhagia (Heavy Menstrual Bleeding)Aizi DwimeilaNo ratings yet
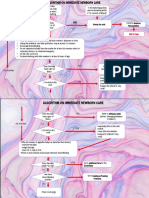
- Immediate Newborn Care AlgorythmDocument2 pagesImmediate Newborn Care AlgorythmMaria Fatima BallezaNo ratings yet
- QuestionsDocument35 pagesQuestionsYasmeen AtiehNo ratings yet
- Untitled Presentation 4Document18 pagesUntitled Presentation 4sumegh sagareNo ratings yet
- Anxiety and Its Relationship WTH Maternal Fetal Attachment in Prgenant Women in Southeast of IranDocument13 pagesAnxiety and Its Relationship WTH Maternal Fetal Attachment in Prgenant Women in Southeast of IranNida Tsaura SNo ratings yet
- Ukn Indonesian College of Obstetrics and GynecologyDocument13 pagesUkn Indonesian College of Obstetrics and GynecologyRizka AdiNo ratings yet
- Gender and LaborDocument2 pagesGender and LaborCenon Paul SeronNo ratings yet
- 2020 06 18 Coronavirus Covid 19 Infection in PregnancyDocument61 pages2020 06 18 Coronavirus Covid 19 Infection in PregnancyIndah AulliaNo ratings yet