You might also like
- End of Life IssuesDocument35 pagesEnd of Life IssuesJeffrey RamosNo ratings yet
- What Is GriefDocument4 pagesWhat Is GriefMarnelie Guerrero AbuanNo ratings yet
- Module 6 Death and DyingDocument38 pagesModule 6 Death and DyingZaren James D. RacaNo ratings yet
- Salcedo-FUNDA LEC 15 End of LIfe CareDocument37 pagesSalcedo-FUNDA LEC 15 End of LIfe CarebaynNo ratings yet
- Martin Caon - Examination Questions and Answers in Basic Anatomy and Physiology 2000 Multiple Choice Questions-Springer (2020)Document746 pagesMartin Caon - Examination Questions and Answers in Basic Anatomy and Physiology 2000 Multiple Choice Questions-Springer (2020)Charles santos da costa100% (6)
- Coping With Loss Death and GrievingDocument33 pagesCoping With Loss Death and Grievingsalmanhabeebek100% (1)
- End of Life CareDocument25 pagesEnd of Life CareMeenu DograNo ratings yet
- Loss Loss Is Any Situation (Actual, Potential, or Perceived) in Which A Valued Object Is ChangedDocument19 pagesLoss Loss Is Any Situation (Actual, Potential, or Perceived) in Which A Valued Object Is ChangedswethashakiNo ratings yet
- Updated Death and DyingDocument35 pagesUpdated Death and DyingGummie Akalal Sugala0% (1)
- End of Life CareDocument12 pagesEnd of Life CaregerajassoNo ratings yet
- Is There Really An Eccentric Action of The Hamstrings During The Swing Phase of High Speed Running? Part I: A Critical Review of The LiteratureDocument11 pagesIs There Really An Eccentric Action of The Hamstrings During The Swing Phase of High Speed Running? Part I: A Critical Review of The LiteratureLuis VargasNo ratings yet
- Loss, Death, and Grieving: Nursing Fundamentals Nurs B20Document19 pagesLoss, Death, and Grieving: Nursing Fundamentals Nurs B20rinkuNo ratings yet
- Hospice CareDocument31 pagesHospice CareQuennie Abellon QuimanNo ratings yet
- What Is Bereavement?Document68 pagesWhat Is Bereavement?deepupopsNo ratings yet
- Presentation - 2 End of Life CareDocument32 pagesPresentation - 2 End of Life CareDaneshwari Sahu100% (1)
- Understanding Death Loss Grief and BereavementDocument29 pagesUnderstanding Death Loss Grief and Bereavementmeldaiska100% (1)
- Concept of Loss, Grieving Death & DyingDocument33 pagesConcept of Loss, Grieving Death & DyingAbdullah Bhatti100% (1)
- Grief, Loss, Death and DyingDocument47 pagesGrief, Loss, Death and DyingRaquel M. MendozaNo ratings yet
- Care of Dying and DeadDocument10 pagesCare of Dying and Deadd1choosenNo ratings yet
- Death & GriefDocument20 pagesDeath & GriefEleanorNo ratings yet
- END OF LIFE CareDocument25 pagesEND OF LIFE Caregireeshsachin100% (1)
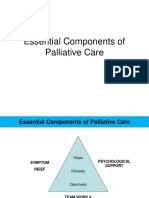
- Essential Components of Palliative CareDocument20 pagesEssential Components of Palliative CareJonah R. Merano60% (5)
- Death Dying and BereavementDocument5 pagesDeath Dying and BereavementImmatureBastardNo ratings yet
- Terminal Illness and DeathDocument37 pagesTerminal Illness and DeathJAYSON KING100% (2)
- Death and Dying: Presented by Dr. Judith SugayDocument21 pagesDeath and Dying: Presented by Dr. Judith SugayMichelle HutamaresNo ratings yet
- Final End of Life CareDocument38 pagesFinal End of Life CareArchana Panika100% (4)
- Acute AppendicitisDocument29 pagesAcute AppendicitisSilhouette Dream100% (1)
- Loss, Death, and Grieving - PPTX 222222-1Document37 pagesLoss, Death, and Grieving - PPTX 222222-1Muhammad Abbas Wali100% (1)
- CHP 43 QuizletDocument3 pagesCHP 43 QuizletJacqueline GreerNo ratings yet
- Grief & Loss Concept Guide Final Copy F23 CBSDocument8 pagesGrief & Loss Concept Guide Final Copy F23 CBSmorganstorey0No ratings yet
- Fundamentals of Nursing OutlineDocument4 pagesFundamentals of Nursing OutlineNina Anne ParacadNo ratings yet
- Dr. Ram Manohar Lohiya National Law University, Lucknow: Death PsychologyDocument11 pagesDr. Ram Manohar Lohiya National Law University, Lucknow: Death PsychologyArpit UpadhyayNo ratings yet
- L14 Reading Reflections Study GuideDocument5 pagesL14 Reading Reflections Study GuideMaria Camila Vangh-egas JNo ratings yet
- Sost - Funda - Coping With LossDocument3 pagesSost - Funda - Coping With LossKYLE SABAYNo ratings yet
- Death and GrievingDocument17 pagesDeath and GrievingAmanda ScarletNo ratings yet
- ObjectivesDocument6 pagesObjectivesLord arainNo ratings yet
- Lesson 3Document4 pagesLesson 3Random RandomNo ratings yet
- Coping With Loss, Death and GrievingDocument43 pagesCoping With Loss, Death and GrievingKishore RathoreNo ratings yet
- End of Life CareDocument19 pagesEnd of Life CareArjumand ZargarNo ratings yet
- Death and DyingDocument3 pagesDeath and DyingHANNAH COLANGONo ratings yet
- Introduction To Palliative Care: by Yonas T. (BSC, MSC)Document64 pagesIntroduction To Palliative Care: by Yonas T. (BSC, MSC)Abdi Mohammed100% (1)
- End of Life Care Workshop ANPDocument34 pagesEnd of Life Care Workshop ANPArjumand ZargarNo ratings yet
- Bereavement in Adult LifeDocument9 pagesBereavement in Adult LifeAzhar MastermindNo ratings yet
- End of Life Issues - EhicsDocument11 pagesEnd of Life Issues - EhicsVenu D DonNo ratings yet
- Topic 4Document11 pagesTopic 4Patricia Mae MurilloNo ratings yet
- Lesson-10 Death and DyingDocument44 pagesLesson-10 Death and Dying2 kidzNo ratings yet
- Group 9 - DYING AND BEREAVEMENTDocument6 pagesGroup 9 - DYING AND BEREAVEMENTRay Sophia CuberoNo ratings yet
- Chapter-29: Care of Terminally Ill PatientDocument92 pagesChapter-29: Care of Terminally Ill PatientMuhammad MuhammadNo ratings yet
- Grief Loss Death Dying: Gerald Rey O. Coquia, RNDocument47 pagesGrief Loss Death Dying: Gerald Rey O. Coquia, RNramzan aliNo ratings yet
- The Dying Process Death Is Defined AsDocument5 pagesThe Dying Process Death Is Defined AsKenn yahweexNo ratings yet
- Legal Definitions of DeathDocument7 pagesLegal Definitions of DeathFatima Diane S. MondejarNo ratings yet
- Coping With Loss, Grieving & DeathDocument19 pagesCoping With Loss, Grieving & DeathDominic SantosNo ratings yet
- End of Life CareDocument21 pagesEnd of Life CareVandana BhasinNo ratings yet
- Introduction MentalDocument48 pagesIntroduction MentalPY 01No ratings yet
- Palliative Dr. WinemakerDocument32 pagesPalliative Dr. WinemakerEzhil Vendhan PalanisamyNo ratings yet
- Care of Terminally Ill Set 2Document36 pagesCare of Terminally Ill Set 2saranya amuNo ratings yet
- What Is GriefDocument10 pagesWhat Is GriefIrene Torshie AttachieNo ratings yet
- Care of Dying PatientDocument22 pagesCare of Dying PatientMANEESH MANINo ratings yet
- Care of Terminally Ill Set 1Document27 pagesCare of Terminally Ill Set 1saranya amuNo ratings yet
- 1 IlnessDocument5 pages1 IlnessY BNo ratings yet
- DefinitionDocument3 pagesDefinitionEhghaa JasmineNo ratings yet
- Coping with Bereavement: A practical guide to getting through griefFrom EverandCoping with Bereavement: A practical guide to getting through griefNo ratings yet
- Undoing Depression: How to Overcome Depression and Anxiety EasilyFrom EverandUndoing Depression: How to Overcome Depression and Anxiety EasilyNo ratings yet
- Introduction To Pakistani SocietyDocument10 pagesIntroduction To Pakistani SocietyAmmar BhattiNo ratings yet
- Biostatics For NursesDocument74 pagesBiostatics For NursesAmmar BhattiNo ratings yet
- Introduction To Diabetes MellitusDocument6 pagesIntroduction To Diabetes MellitusAmmar BhattiNo ratings yet
- 1 Perspective of Paediatric NursingDocument5 pages1 Perspective of Paediatric NursingAmmar BhattiNo ratings yet
- UNIT III Disorders of Neurological SystemDocument7 pagesUNIT III Disorders of Neurological SystemAmmar BhattiNo ratings yet
- Cardiovascular DisordersDocument6 pagesCardiovascular DisordersAmmar BhattiNo ratings yet
- Nitrogenase - WikipediaDocument8 pagesNitrogenase - WikipediafoonganNo ratings yet
- Muscle Spindle: Name: Rishbha Tiku Year:3 Semester:6Document9 pagesMuscle Spindle: Name: Rishbha Tiku Year:3 Semester:6Rishbha TikuNo ratings yet
- Mark Scheme Paper 1B June 2014Document17 pagesMark Scheme Paper 1B June 2014Shovon MorshedNo ratings yet
- Current Management Trends in Sickle Cell DiseaseDocument51 pagesCurrent Management Trends in Sickle Cell DiseaseJohn chuksNo ratings yet
- MY Bio 12 Photosynthesis AssignmentDocument6 pagesMY Bio 12 Photosynthesis AssignmentGSemenkovaNo ratings yet
- Microbios Intestinales en Trastornos Neurocognitivos y de Salud Mental (Halversona y Alagiakrishnan, 2020)Document21 pagesMicrobios Intestinales en Trastornos Neurocognitivos y de Salud Mental (Halversona y Alagiakrishnan, 2020)Centro integral del desarrollo LogrosNo ratings yet
- Passive & Active TransportDocument31 pagesPassive & Active TransportToni - Ann IrvingNo ratings yet
- Addressing Patient Specificity in The Engineering of Tumor ModelsDocument36 pagesAddressing Patient Specificity in The Engineering of Tumor ModelsNadia Al RefaieNo ratings yet
- Chase Kinsey CVDocument7 pagesChase Kinsey CVapi-637234536No ratings yet
- ONLINE - Lab 1 - Language of AnatomyDocument9 pagesONLINE - Lab 1 - Language of AnatomyaliNo ratings yet
- Pinnularia PresentationDocument10 pagesPinnularia PresentationIjaz Ahmed100% (1)
- Rempe 2007Document5 pagesRempe 2007aristyadewi414No ratings yet
- Biology 9 Icse Sample Paper 10Document5 pagesBiology 9 Icse Sample Paper 10Vivaan GandhiNo ratings yet
- Chapter 14 - Coordination and Response NoteDocument17 pagesChapter 14 - Coordination and Response NoteShort FilmsNo ratings yet
- Excretory Products and Their EliminationDocument13 pagesExcretory Products and Their Eliminationaravind kishanNo ratings yet
- d04574 26 Value Sheet Utrol MuDocument3 pagesd04574 26 Value Sheet Utrol MuAvicenne ZagoraNo ratings yet
- TESTIS CELL BIOLOGY Spermatozoa and Sperm Structure Auger 2018Document6 pagesTESTIS CELL BIOLOGY Spermatozoa and Sperm Structure Auger 2018LudimilaNo ratings yet
- Apple Seed DormancyDocument8 pagesApple Seed DormancyMUHAMMAD FIRDAUS BIN AMIR HUSINNo ratings yet
- Unit 6: Enzymes: Image Modified From " ," by Openstax College, BiologyDocument4 pagesUnit 6: Enzymes: Image Modified From " ," by Openstax College, BiologyAbraham BanjoNo ratings yet
- BioPsy 1 - Intro To BioPsyDocument4 pagesBioPsy 1 - Intro To BioPsyTim AroscoNo ratings yet
- AD0460447Document26 pagesAD0460447Mario ColliNo ratings yet
- G5 - Ls3The Skeletaland Muscular System - Worksheet3Document4 pagesG5 - Ls3The Skeletaland Muscular System - Worksheet3ak dNo ratings yet
- Hypoxemic Respiratory FailureDocument70 pagesHypoxemic Respiratory FailureMohamed Rikarz Ahamed RikarzNo ratings yet
- Pharmacology: Pharmacokinetics - Part 1Document9 pagesPharmacology: Pharmacokinetics - Part 1RodrigoNo ratings yet
- Baddeley 2000 EvaluationDocument9 pagesBaddeley 2000 Evaluationteng yewwNo ratings yet
- Biology Class 9 Kerala Notes Part 1 (English Medium) by OdakkalDocument13 pagesBiology Class 9 Kerala Notes Part 1 (English Medium) by Odakkalmariyu palakkot tms100% (5)
- Stem 2c-Music On Plant Growth FinalDocument91 pagesStem 2c-Music On Plant Growth FinalYonaNo ratings yet