You might also like
- MBR 2019 - Anes ENT Ophtha HandoutsDocument17 pagesMBR 2019 - Anes ENT Ophtha HandoutsNica Lopez FernandezNo ratings yet
- Pharmacology of Anaesthetic Agents II: Inhalation Anaesthetic AgentsDocument6 pagesPharmacology of Anaesthetic Agents II: Inhalation Anaesthetic AgentsAna Lucia SaavedraNo ratings yet
- Spinal Mechanisms of Pain and Analgesia: ReviewarticleDocument17 pagesSpinal Mechanisms of Pain and Analgesia: ReviewarticleAblfazl KianiNo ratings yet
- Non-Opioid Analgesics: Learning ObjectivesDocument4 pagesNon-Opioid Analgesics: Learning ObjectivesIndah NisaNo ratings yet
- Update of OpioidDocument5 pagesUpdate of OpioidFieska AzizahNo ratings yet
- Pharmacology of Anaesthetic Agents II: Inhalation Anaesthetic AgentsDocument6 pagesPharmacology of Anaesthetic Agents II: Inhalation Anaesthetic Agentsmouxritsa_83No ratings yet
- Intrathecal MorphineDocument6 pagesIntrathecal MorphineJoana MoreiraNo ratings yet
- Inhalasi Jurnal 1Document6 pagesInhalasi Jurnal 1Fanhy liebe smartNo ratings yet
- MKT 038Document6 pagesMKT 038peter_soósNo ratings yet
- Pharmacology of Anaesthetic Agents II Inhalation ADocument7 pagesPharmacology of Anaesthetic Agents II Inhalation AMarsya Yulinesia LoppiesNo ratings yet
- Pharmacology of Anaesthetic Agents II Inhalation ADocument7 pagesPharmacology of Anaesthetic Agents II Inhalation AmunaNo ratings yet
- Httpsscielo Isciii Espdfdolorv19n2revisionmbe PDFDocument23 pagesHttpsscielo Isciii Espdfdolorv19n2revisionmbe PDFJoelGámezNo ratings yet
- Kee 1998 Intrathecal Pethidine Pharmacology and Clinical ApplicationsDocument10 pagesKee 1998 Intrathecal Pethidine Pharmacology and Clinical ApplicationsCarlos DelgadoNo ratings yet
- A Comparative Study of Low Dose Hyperbaric Bupivacine With Fentanyl and Hyperbaric Bupivacaine in Spinal Anaesthesia For Below Umbilical SurgeriesDocument1 pageA Comparative Study of Low Dose Hyperbaric Bupivacine With Fentanyl and Hyperbaric Bupivacaine in Spinal Anaesthesia For Below Umbilical SurgeriesTahirNo ratings yet
- 1992 M. LOEFFLER, - Oral Benzodiazepines and Conscious Sedation - A Review PAULDocument9 pages1992 M. LOEFFLER, - Oral Benzodiazepines and Conscious Sedation - A Review PAULAlejandro RuizNo ratings yet
- 1.epinfrina y Efecto CerebralDocument13 pages1.epinfrina y Efecto Cerebralheiddy MendozaNo ratings yet
- HIPOFISIS1Document4 pagesHIPOFISIS1isela castroNo ratings yet
- Central Pain ModulatingDocument9 pagesCentral Pain ModulatingSebastiano SerraNo ratings yet
- LECTURADocument13 pagesLECTURAKaren VillegasNo ratings yet
- Pharmacology of Anaesthetic Agents I: Intravenous Anaesthetic AgentsDocument6 pagesPharmacology of Anaesthetic Agents I: Intravenous Anaesthetic Agentsmouxritsa_83No ratings yet
- Opioid Adjuvant in NeuraxialDocument10 pagesOpioid Adjuvant in NeuraxialiswanlatifNo ratings yet
- A Comparative Study of Intrathecal Injection of Bupivacaine Alone or With Fentanyl, Clonidine, and Neostigmine in Lower Abdominal SurgeriesDocument16 pagesA Comparative Study of Intrathecal Injection of Bupivacaine Alone or With Fentanyl, Clonidine, and Neostigmine in Lower Abdominal SurgeriesdhiyaNo ratings yet
- PhenylephrineDocument17 pagesPhenylephrineBrin DaNo ratings yet
- Fisiologia de Los Opioides Epidurales e IntratectalesDocument13 pagesFisiologia de Los Opioides Epidurales e Intratectalessanjuandediosanestesia100% (5)
- 2007 Inadvertent Intrathecal Vincristine AdministrationDocument4 pages2007 Inadvertent Intrathecal Vincristine AdministrationDaniela MéndezNo ratings yet
- Serotonin-Based Pharmacotherapy For Acute Neuroleptic-Induced Akathisia A New Approach To An Old Problem - Michael PoyurovskyDocument5 pagesSerotonin-Based Pharmacotherapy For Acute Neuroleptic-Induced Akathisia A New Approach To An Old Problem - Michael PoyurovskyFábio Yutani KosekiNo ratings yet
- Analgesicos No OpioidesDocument4 pagesAnalgesicos No OpioidesBelén OchoaNo ratings yet
- Biomedicines: Peripheral Nerve Stimulation: The Evolution in Pain MedicineDocument4 pagesBiomedicines: Peripheral Nerve Stimulation: The Evolution in Pain MedicineGiancarlo Gardella MartínezNo ratings yet
- Neuraxial Agents: Robert W. Hurley Dustin Anderson Steven P. CohenDocument1 pageNeuraxial Agents: Robert W. Hurley Dustin Anderson Steven P. CohenFaith Acu CureNo ratings yet
- Chapt 3Document5 pagesChapt 3Javier Farias VeraNo ratings yet
- Pharmacology OpioidDocument58 pagesPharmacology OpioidCitra Wulandari SofyanNo ratings yet
- Anesthetics Fa 2022Document4 pagesAnesthetics Fa 2022Assanov AibekNo ratings yet
- Study AssignmentDocument11 pagesStudy AssignmentThe LegendaryCarrotMasterNo ratings yet
- Hypnosis and Cingulate-Mediated Mechanisms of AnalgesiaDocument20 pagesHypnosis and Cingulate-Mediated Mechanisms of AnalgesiaCristian GondacNo ratings yet
- Perineural Adjuncts For Peripheral Nerve BlockDocument7 pagesPerineural Adjuncts For Peripheral Nerve BlockpitriaNo ratings yet
- Central Nervous System Targets: Supraspinal Mechanisms of AnalgesiaDocument7 pagesCentral Nervous System Targets: Supraspinal Mechanisms of AnalgesiaamelietunNo ratings yet
- Sacral Burst Neuromodulation Via Caudal Approach As A Treatment For Chronic CoccydyniaDocument3 pagesSacral Burst Neuromodulation Via Caudal Approach As A Treatment For Chronic CoccydyniaromanciviNo ratings yet
- Addition of Morphine To Local Anesthetic Infiltration Does Not Improve Analgesia After Pediatric Dental ExtractionsDocument5 pagesAddition of Morphine To Local Anesthetic Infiltration Does Not Improve Analgesia After Pediatric Dental Extractionsمحمد عبدالرحمنNo ratings yet
- Anesthesia in Surgical PTS 1Document41 pagesAnesthesia in Surgical PTS 1Minale MenberuNo ratings yet
- Eps Opioid WithdrawalDocument2 pagesEps Opioid WithdrawalPuneetNo ratings yet
- Neural Circuits of Anxiolytic and Antidepressant Pherine MoleculesDocument7 pagesNeural Circuits of Anxiolytic and Antidepressant Pherine MoleculesNaiana PaulaNo ratings yet
- Spinal Anaesthesia For Ambulatory Arthroscopic Surgery of The KneeDocument6 pagesSpinal Anaesthesia For Ambulatory Arthroscopic Surgery of The KneeGustavo MosqueraNo ratings yet
- DOR - FENOL - Chemical Ablation of Genicular Nerve With Phenol For Pain Relief in Patients With Knee Osteoarthritis A Prospective Study - CompressedDocument7 pagesDOR - FENOL - Chemical Ablation of Genicular Nerve With Phenol For Pain Relief in Patients With Knee Osteoarthritis A Prospective Study - CompressedGustavo FredericoNo ratings yet
- Inhalation Anesthetic Drug StudyDocument4 pagesInhalation Anesthetic Drug StudyElisse RodulfoNo ratings yet
- New Developments in The Management of NarcolepsyDocument19 pagesNew Developments in The Management of Narcolepsypeppers226647dndsh34No ratings yet
- 5 Cannabis Smoke & PsychoacousticsDocument12 pages5 Cannabis Smoke & PsychoacousticsJorge E. Azanza BacaNo ratings yet
- UntitledDocument19 pagesUntitledSarbjeet SinghNo ratings yet
- Peripheral Mechanisms of Opioid Analgesia: Christoph Stein and Leonie Julia LangDocument6 pagesPeripheral Mechanisms of Opioid Analgesia: Christoph Stein and Leonie Julia LangLidiaNo ratings yet
- Ijca 7 2 313 318Document6 pagesIjca 7 2 313 318Bianca CaterinalisendraNo ratings yet
- Review Article: Pathic Association Published A Supplement Dedicated To EndorDocument15 pagesReview Article: Pathic Association Published A Supplement Dedicated To EndorClark DNo ratings yet
- Wei Et Al 2015 Endocannabinoid Signaling Mediates Oxytocin Driven Social RewardDocument6 pagesWei Et Al 2015 Endocannabinoid Signaling Mediates Oxytocin Driven Social RewarddhammanautaNo ratings yet
- Pivotal Role of Carnosine in The Modulation of Brain Cells ActivityDocument19 pagesPivotal Role of Carnosine in The Modulation of Brain Cells ActivityDaniel Stefano Vásquez RojasNo ratings yet
- Mepivacaine Vs BupivacaineDocument11 pagesMepivacaine Vs Bupivacainetia astrianaNo ratings yet
- 2014 EJA, Ondansetron Oculogyric CrisisDocument2 pages2014 EJA, Ondansetron Oculogyric CrisisAirwayNo ratings yet
- Panophthalmoplegia and Vision Loss After Cosmetic Nasal Dorsum InjectionDocument3 pagesPanophthalmoplegia and Vision Loss After Cosmetic Nasal Dorsum InjectionKerlida SantosNo ratings yet
- Journal Course Evidence Based Use of Nonopioid Analgesics August 2018Document7 pagesJournal Course Evidence Based Use of Nonopioid Analgesics August 2018DesywinNo ratings yet
- An Approach To Anisocoria.4Document7 pagesAn Approach To Anisocoria.4FrancescFranquesaNo ratings yet
- 677 FullDocument5 pages677 FullNoniqTobingNo ratings yet
- Neuronal Information TransferFrom EverandNeuronal Information TransferArthur KarlinNo ratings yet
- Physiol 93 B3Document1 pagePhysiol 93 B3DonkeyManNo ratings yet
- Pharm 02 A10Document2 pagesPharm 02 A10DonkeyManNo ratings yet
- CEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDocument5 pagesCEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDonkeyManNo ratings yet
- CEACCP - Latex AllergyDocument4 pagesCEACCP - Latex AllergyDonkeyManNo ratings yet
- CEACCP - KetamineDocument5 pagesCEACCP - KetamineDonkeyManNo ratings yet
- Pharm 02 A11Document4 pagesPharm 02 A11DonkeyManNo ratings yet
- Pharm 00 B11Document1 pagePharm 00 B11DonkeyManNo ratings yet
- Pharm 00 A12Document1 pagePharm 00 A12DonkeyManNo ratings yet
- Pharm 00 B15Document2 pagesPharm 00 B15DonkeyManNo ratings yet
- Pharm 00 B14Document2 pagesPharm 00 B14DonkeyManNo ratings yet
- Pharm 00 A14Document2 pagesPharm 00 A14DonkeyManNo ratings yet
- Pharm 00 A9Document2 pagesPharm 00 A9DonkeyManNo ratings yet
- Pharm 00 A15Document2 pagesPharm 00 A15DonkeyManNo ratings yet
- Compare and Contrast Neostigmine and The Organophosphate CompoundsDocument1 pageCompare and Contrast Neostigmine and The Organophosphate CompoundsDonkeyManNo ratings yet
- Outline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDocument2 pagesOutline The Physiological Consequences of Hyperosmolar Diabetic KetoacidosisDonkeyManNo ratings yet
- Compare and Contrast The Pharamcology of Ephedrine and NoradrenalineDocument1 pageCompare and Contrast The Pharamcology of Ephedrine and NoradrenalineDonkeyManNo ratings yet
- Define The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDocument2 pagesDefine The Mechanisms of Action and Adverse Effects of Metoprolol, GTN, and Diltiazem When Used To Manage MIDonkeyManNo ratings yet
- Palliative Care HandbookDocument82 pagesPalliative Care HandbookDonkeyManNo ratings yet
- Compare and Contrast The Pharmacology of Esmolol and PropanololDocument1 pageCompare and Contrast The Pharmacology of Esmolol and PropanololDonkeyManNo ratings yet
- VOLATILEAGENTSDocument4 pagesVOLATILEAGENTSDonkeyManNo ratings yet
- Comparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871Document7 pagesComparative Pharmacokinetics of Fentanyl and Alfentanil: Br. J. Anaesth. (1982), 54, 871DonkeyManNo ratings yet
- Compare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDocument2 pagesCompare and Contrast Atropine and Glycopyrulate, and Discuss The Clinical ImplicationsDonkeyManNo ratings yet
- Base Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDocument1 pageBase Excess (Be) Measure of Metabolic Acid-Base Status: Dr. David LynessDonkeyManNo ratings yet
- FS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018Document4 pagesFS Antimicrobial Dosing Obesity AMS Updates Issue4 - Nov2018DonkeyManNo ratings yet
- Cholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDocument4 pagesCholinergic Agents: Cholinergic Receptors Types of Receptor Muscarinic Receptor Nicotinic ReceptorDonkeyManNo ratings yet
- The Physiology of The GIT and The Liver QuestionsDocument44 pagesThe Physiology of The GIT and The Liver QuestionsDonkeyManNo ratings yet
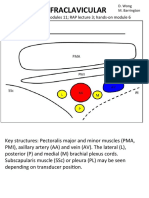
- Infraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6Document4 pagesInfraclavicular: Toolbox: Online Modules 11 RAP Lecture 3 Hands - On Module 6DonkeyManNo ratings yet
- Bio Resonance Therapy For ParasitesDocument7 pagesBio Resonance Therapy For ParasitesMiyuriT100% (3)
- Personal Decisions Are The Leading Cause of Death PDFDocument13 pagesPersonal Decisions Are The Leading Cause of Death PDFLan HươngNo ratings yet
- Aphasia AssessmentDocument7 pagesAphasia AssessmentMarliani AfriastutiNo ratings yet
- OclusiónDocument6 pagesOclusiónANDREA ISABELLA MATACHIONE ROMERONo ratings yet
- ETT Vs LMADocument33 pagesETT Vs LMAitaindrianiNo ratings yet
- Health Benifits of YogasanaDocument4 pagesHealth Benifits of YogasanaCcywi CcywiNo ratings yet
- Joubert Syndrome Jbts / Cerebellooculorenal Syndrome: Clinical SynopsisDocument2 pagesJoubert Syndrome Jbts / Cerebellooculorenal Syndrome: Clinical SynopsisBlueash BehNo ratings yet
- Review Article Intrathecal Drug Spread: G. Hocking and J. A. W. WildsmithDocument11 pagesReview Article Intrathecal Drug Spread: G. Hocking and J. A. W. WildsmithHalim SudonoNo ratings yet
- Cardiac Computed TomographyDocument29 pagesCardiac Computed TomographyAnu MavelyNo ratings yet
- Mumbai Claim FormDocument5 pagesMumbai Claim FormsunsangraNo ratings yet
- Current Concepts in Lower Extremity Reconstruction.36Document15 pagesCurrent Concepts in Lower Extremity Reconstruction.36Aura RivasNo ratings yet
- Gengigel For GingivitisDocument7 pagesGengigel For GingivitisIka Dewi RahmawatiNo ratings yet
- Visual Anosognosia (Anton-Babinski Syndrome) : Report of Two Cases Associated With Ischemic Cerebrovascular DiseaseDocument5 pagesVisual Anosognosia (Anton-Babinski Syndrome) : Report of Two Cases Associated With Ischemic Cerebrovascular DiseaseHanna EnitaNo ratings yet
- Questions and AnswerDocument5 pagesQuestions and AnswerPatricia Camille Ponce JonghunNo ratings yet
- Create PDFDocument92 pagesCreate PDFSri muyaroahNo ratings yet
- Recurrent/Persistent Pneumonia Among Children in Upper EgyptDocument14 pagesRecurrent/Persistent Pneumonia Among Children in Upper EgyptLaila Ninda ShofiaNo ratings yet
- Internal Medicine 5th MidtermDocument13 pagesInternal Medicine 5th MidtermIashdip iashdipNo ratings yet
- SchistosomiasisDocument3 pagesSchistosomiasisglaire927No ratings yet
- Med Surg Medication Study GuideDocument8 pagesMed Surg Medication Study Guidetina100% (1)
- Diagnosis Procedure: DRG Sri Rezeki, SP - PMDocument94 pagesDiagnosis Procedure: DRG Sri Rezeki, SP - PMNiska DarliantiNo ratings yet
- Sample Chapter 9780323399562Document23 pagesSample Chapter 9780323399562TaeyomiNo ratings yet
- Review of Biguanide (Metformin) Toxicity: George Sam Wang, MD and Christopher Hoyte, MDDocument14 pagesReview of Biguanide (Metformin) Toxicity: George Sam Wang, MD and Christopher Hoyte, MDIoana IonescuNo ratings yet
- Cirrhosis of LiverDocument7 pagesCirrhosis of LivermOHAN.S100% (3)
- 8BreathingExercises Calmhappyhealthy PDFDocument10 pages8BreathingExercises Calmhappyhealthy PDFlunn100% (1)
- NCM 103 Chapter 36 Skin Integrity and Wound Care (Canvas)Document121 pagesNCM 103 Chapter 36 Skin Integrity and Wound Care (Canvas)AinaB ManaloNo ratings yet
- NCP: Alcohol Acute WithdrawlDocument11 pagesNCP: Alcohol Acute WithdrawlJavie100% (2)
- Adult Health Final Study GuideDocument5 pagesAdult Health Final Study GuideNurseNancy93100% (1)
- Letter - Physical ExamDocument6 pagesLetter - Physical ExamLaurence LesmorasNo ratings yet
- Inflammatory Bowel Disease FinalDocument60 pagesInflammatory Bowel Disease FinalRawabi rawabi1997No ratings yet
- Supply Disruption AlertDocument5 pagesSupply Disruption AlertM Teresa LeivaNo ratings yet