You might also like
- 2020 - A New Vision A Future For Regenerative MedicineDocument33 pages2020 - A New Vision A Future For Regenerative MedicineGiulianoNo ratings yet
- The Meat MarketDocument4 pagesThe Meat Marketasha328No ratings yet
- Cash For Kidneys: The Case For A Market For OrgansDocument5 pagesCash For Kidneys: The Case For A Market For OrganssepulNo ratings yet
- Organ Sales Will Save LivesDocument4 pagesOrgan Sales Will Save Livesapi-534778534No ratings yet
- Richie Organ DonationDocument36 pagesRichie Organ DonationHema TNo ratings yet
- Organs 8Document11 pagesOrgans 8api-396542988No ratings yet
- Organ Donation: An Important DecisionDocument2 pagesOrgan Donation: An Important DecisionAntonio BerebereNo ratings yet
- Market For KidneysDocument11 pagesMarket For Kidneysapi-605344411No ratings yet
- Transplantation: J. Med. EthicsDocument3 pagesTransplantation: J. Med. EthicsFuraya FuisaNo ratings yet
- Organ TransplantationDocument25 pagesOrgan Transplantationb29ondNo ratings yet
- 8organ DonationDocument14 pages8organ DonationLoikan JosueNo ratings yet
- Organ Donation Is The Removal of TheDocument8 pagesOrgan Donation Is The Removal of TheAdhavan KnkNo ratings yet
- One Chance in A Million AltruismDocument43 pagesOne Chance in A Million AltruismJoBPNo ratings yet
- Don't Let High-Minded Ideals Get in The Way of Saving Lives By: Jesse KlineDocument2 pagesDon't Let High-Minded Ideals Get in The Way of Saving Lives By: Jesse KlineViona DamayantiNo ratings yet
- Organ DonationDocument34 pagesOrgan Donationapi-404314061No ratings yet
- Organ DonationDocument25 pagesOrgan DonationNazatulJuhariNo ratings yet
- Opt in or Opt OutDocument3 pagesOpt in or Opt OutIrina IonescuNo ratings yet
- BuzzleDocument4 pagesBuzzledobosionelaNo ratings yet
- The Global Organ Shortage: Economic Causes, Human Consequences, Policy ResponsesFrom EverandThe Global Organ Shortage: Economic Causes, Human Consequences, Policy ResponsesNo ratings yet
- Should Everyone Be Expected To Donate Suitable Organs After Death - DadDocument2 pagesShould Everyone Be Expected To Donate Suitable Organs After Death - DadwongkmjasonNo ratings yet
- Human Organ Sales Research PaperDocument7 pagesHuman Organ Sales Research Papercammtpw6100% (1)
- Euthanasia WinnersDocument2 pagesEuthanasia WinnersPedro Abraham Cruz CruzNo ratings yet
- Answers To Section 3.7 Organ TransplantationDocument2 pagesAnswers To Section 3.7 Organ TransplantationbrownieallennNo ratings yet
- Transplantation-Ethical IssuesDocument17 pagesTransplantation-Ethical IssuesivkovictNo ratings yet
- Organ TraffickingDocument48 pagesOrgan TraffickingSpencer Venable100% (1)
- Organ Donation PresentationDocument40 pagesOrgan Donation PresentationKryza Dale Bunado Batican100% (1)
- Organ TransplantationDocument33 pagesOrgan TransplantationAyyagariKathyayani100% (1)
- Organ Donation EssayDocument6 pagesOrgan Donation EssayOscar Javier Rodríguez UribeNo ratings yet
- Killing For OrgansDocument3 pagesKilling For Organsjadawgis7322288No ratings yet
- April 29 Asynch TaskDocument14 pagesApril 29 Asynch TaskMhartin SortonisNo ratings yet
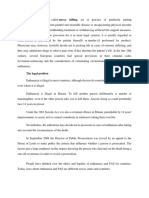
- Euthanasia, Also Called Mercy Killing, Act or Practice of Painlessly PuttingDocument7 pagesEuthanasia, Also Called Mercy Killing, Act or Practice of Painlessly PuttingtaetaelandingNo ratings yet
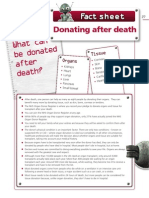
- Fact Sheet Donating After DeathDocument1 pageFact Sheet Donating After DeathMauETNo ratings yet
- Policy Debate-Should There Be A Market For Human OrgansDocument6 pagesPolicy Debate-Should There Be A Market For Human OrgansSalman KhanNo ratings yet
- Research PaperDocument7 pagesResearch Paperapi-366892152No ratings yet
- Stats - CFM: ReferrenceDocument7 pagesStats - CFM: ReferrenceMunawwarah IsmailNo ratings yet
- Draft Visual Analysis EssayDocument5 pagesDraft Visual Analysis Essayapi-322143619No ratings yet
- Commerce in Organs Has Led To Human Rights Violations: Desperation and GreedDocument5 pagesCommerce in Organs Has Led To Human Rights Violations: Desperation and GreedJenAldrovandiNo ratings yet
- Emily Risner - Research Essay PDFDocument10 pagesEmily Risner - Research Essay PDFapi-455396636No ratings yet
- The Development of Science and Organ Donation - Abin AndrewsDocument4 pagesThe Development of Science and Organ Donation - Abin AndrewsABIN ANDREWS BNo ratings yet
- Many Sleepless Nights: The World of Organ TransplantationFrom EverandMany Sleepless Nights: The World of Organ TransplantationRating: 3 out of 5 stars3/5 (1)
- Lecture 4.1Document55 pagesLecture 4.1gokulkrishnayadhavNo ratings yet
- Kidney ExchangeDocument47 pagesKidney Exchangej2003.thomasNo ratings yet
- Organ Donation - BamsDocument33 pagesOrgan Donation - BamsMuhammad AL HafizhNo ratings yet
- Organ Sale and DonationDocument61 pagesOrgan Sale and DonationSachin PatelNo ratings yet
- Flynn Et Al v. Eric Holder Et AlDocument18 pagesFlynn Et Al v. Eric Holder Et AlDoug MataconisNo ratings yet
- The Benefits and Implications of A Legalized Organ Sales SystemDocument10 pagesThe Benefits and Implications of A Legalized Organ Sales Systemapi-466408724100% (1)
- Article AJTCompensationof DonorDocument10 pagesArticle AJTCompensationof DonorPrisa DeliaNo ratings yet
- Lecture 5Document72 pagesLecture 5gokulkrishnayadhavNo ratings yet
- Organ DonationDocument3 pagesOrgan DonationGrant DonovanNo ratings yet
- Legalization of Organ SaleDocument5 pagesLegalization of Organ Saleapi-285784432No ratings yet
- Don't Sell Your Organs: A Legal Analysis of Organ Donations. Brittany N. Welsh First Colonial High SchoolDocument20 pagesDon't Sell Your Organs: A Legal Analysis of Organ Donations. Brittany N. Welsh First Colonial High Schoolapi-449622457No ratings yet
- Challenges in Organ TransplantationDocument10 pagesChallenges in Organ TransplantationBrie100% (1)
- Organ Transplantation PowerpointDocument23 pagesOrgan Transplantation PowerpointLawrenz PendeltonNo ratings yet
- Cause and Effect EssayDocument8 pagesCause and Effect Essaybonnie reeseNo ratings yet
- Organ Sale Research PaperDocument8 pagesOrgan Sale Research Papernikuvivakuv3100% (1)
- In Defense of A Regulated Market in Kidneys From Living VendorsDocument35 pagesIn Defense of A Regulated Market in Kidneys From Living VendorssemeluseNo ratings yet
- Research Paper Organ SaleDocument5 pagesResearch Paper Organ Salepukjkzplg100% (1)
- Organ Trafficking PaperDocument26 pagesOrgan Trafficking Papermcris101100% (1)
- Organ Transplant Thesis StatementDocument7 pagesOrgan Transplant Thesis Statementafcmayfzq100% (2)
- Awareness of Legislation Moderates The Effect of Opt-Out Consent On Organ Donation IntentionsDocument6 pagesAwareness of Legislation Moderates The Effect of Opt-Out Consent On Organ Donation IntentionsVictoriaNo ratings yet
- Organ Donation ModuleDocument4 pagesOrgan Donation ModuleMegs Jugueta EstebanNo ratings yet
- MIS ch04 2024Document11 pagesMIS ch04 2024Imen KsouriNo ratings yet
- FinalDocument3 pagesFinalImen KsouriNo ratings yet
- Sampling and Sampling DistributionsDocument5 pagesSampling and Sampling DistributionsImen KsouriNo ratings yet
- Formulation HomeworkDocument2 pagesFormulation HomeworkImen KsouriNo ratings yet
- Bop Excel ConnectionDocument22 pagesBop Excel ConnectionImen KsouriNo ratings yet
- Stat 2 HomeworkDocument5 pagesStat 2 HomeworkImen KsouriNo ratings yet
- Assignment 4 StatDocument3 pagesAssignment 4 StatImen KsouriNo ratings yet
- Legal and Ethical Aspects in NursingDocument35 pagesLegal and Ethical Aspects in NursingSalman HabeebNo ratings yet
- F.6 (1) 2013 12 01 2016Document111 pagesF.6 (1) 2013 12 01 2016atipriya choudharyNo ratings yet
- Donate Life - Organ Donation Frequently Asked QuestionsDocument4 pagesDonate Life - Organ Donation Frequently Asked QuestionsAdrian ButlerNo ratings yet
- Organ TraffickingDocument5 pagesOrgan TraffickingShraddha ReddyNo ratings yet
- C2 - Evaluarea PretransplantDocument31 pagesC2 - Evaluarea PretransplantIuliia •No ratings yet
- Should Everyone Be Expected To Donate Suitable Organs After Death - DadDocument2 pagesShould Everyone Be Expected To Donate Suitable Organs After Death - DadwongkmjasonNo ratings yet
- Appreciation For A Second Chance: Rreeffiinneerryy FfiirreeDocument28 pagesAppreciation For A Second Chance: Rreeffiinneerryy FfiirreeSan Mateo Daily JournalNo ratings yet
- Eurotransplant: Zoë Daudey - Biology - 11-12-2017 - A1EDocument10 pagesEurotransplant: Zoë Daudey - Biology - 11-12-2017 - A1Eapi-390089783No ratings yet
- 3) Case Study - DATRIDocument2 pages3) Case Study - DATRIAdarsh UnnyNo ratings yet
- TB3BIOANDGEOUND1Document10 pagesTB3BIOANDGEOUND1Núria Real TortosaNo ratings yet
- Tort Submission GuidelinesDocument9 pagesTort Submission GuidelinesANKITHA IYERNo ratings yet
- By Paul Pearsall, PHD Gary E. Schwartz, PHD Linda G. Russek, PHDDocument8 pagesBy Paul Pearsall, PHD Gary E. Schwartz, PHD Linda G. Russek, PHDJOSH USHERNo ratings yet
- Easy-Health Policy-Wording Standard PDFDocument21 pagesEasy-Health Policy-Wording Standard PDFdeepak_singla227No ratings yet
- Taxation Challenge - With Answer KeyDocument9 pagesTaxation Challenge - With Answer Keyariaseg100% (1)
- 2016 - Long-Term Donor Outcomes After Pure Laparoscopic Versus Open Living Donor NephrectomyDocument7 pages2016 - Long-Term Donor Outcomes After Pure Laparoscopic Versus Open Living Donor Nephrectomynarutota181No ratings yet
- Nurse Anesthesia-Saunders - Elsevier (2017) - Copy 12Document176 pagesNurse Anesthesia-Saunders - Elsevier (2017) - Copy 12Marsel DonaNo ratings yet
- Application of Biology (ZOOLOGY)Document10 pagesApplication of Biology (ZOOLOGY)md dtlNo ratings yet
- Lopa Media KitDocument6 pagesLopa Media Kitapi-537073027No ratings yet
- Classroom Activity 5cDocument2 pagesClassroom Activity 5cAgo FunesNo ratings yet
- LDLF Press Release 20012 Swabs For 2012Document2 pagesLDLF Press Release 20012 Swabs For 2012Luis Danvers Leukemia FundNo ratings yet
- Kidney Transplant: Mrs - Linta Thomas Assistant Professor KihsDocument19 pagesKidney Transplant: Mrs - Linta Thomas Assistant Professor KihsLintaNo ratings yet
- Withdrawal of Objection FormDocument1 pageWithdrawal of Objection FormNur Ain Mohd AminNo ratings yet
- Bioethics - Lesson 5Document13 pagesBioethics - Lesson 5Flonamae AbiarNo ratings yet
- Organ Transplantation PowerpointDocument23 pagesOrgan Transplantation PowerpointLawrenz PendeltonNo ratings yet
- Organ Transplantation and DonationDocument5 pagesOrgan Transplantation and Donationsarguss14100% (1)
- Legal and Ethical Aspects of Critical Care NursingDocument66 pagesLegal and Ethical Aspects of Critical Care NursingJamille Abenir Lopez100% (2)
- List of Senate BillsDocument18 pagesList of Senate BillsLouie SantosNo ratings yet
- 9 Moral Dilemmas That Will Break Your BrainDocument11 pages9 Moral Dilemmas That Will Break Your BrainMary Charlene ValmonteNo ratings yet
- Reviewer in Ethics (Finals)Document11 pagesReviewer in Ethics (Finals)Justeen BalcortaNo ratings yet