You might also like
- Artritis Reactiva Por Chlamydia TrachomatisDocument3 pagesArtritis Reactiva Por Chlamydia TrachomatisSomtusNo ratings yet
- Jaqt 06 I 3 P 203Document2 pagesJaqt 06 I 3 P 203Dewi LarasatiiNo ratings yet
- Streptococcal Pharyngitis-Rapid Diagnosis by Stain: Gram Subhash C. Sharma P. V. SubbukrishnanDocument3 pagesStreptococcal Pharyngitis-Rapid Diagnosis by Stain: Gram Subhash C. Sharma P. V. Subbukrishnanigobythename AJNo ratings yet
- Jurnal THDocument13 pagesJurnal THasa mutiaNo ratings yet
- Fig. 1 Fig. 1: Correspondence Pathology (2019), 51 (4), JuneDocument3 pagesFig. 1 Fig. 1: Correspondence Pathology (2019), 51 (4), JuneDiego TulcanNo ratings yet
- The Use of Levofloxacin in A Patient With Leptospirosis (#610928) - 793160Document2 pagesThe Use of Levofloxacin in A Patient With Leptospirosis (#610928) - 793160Emmanuel MorilloNo ratings yet
- Conflict of Interests: Aspergilosis Cutánea Secundaria Pustulosa en Paciente InmunosuprimidoDocument4 pagesConflict of Interests: Aspergilosis Cutánea Secundaria Pustulosa en Paciente InmunosuprimidoJuana de los Milagros Chiroque Zeta.No ratings yet
- Peled 2004Document2 pagesPeled 2004drpranaykumar5529No ratings yet
- Diagnostic Polymerase Chain Reaction For DonovanosDocument3 pagesDiagnostic Polymerase Chain Reaction For DonovanosSheilaNo ratings yet
- Faustino 2008Document7 pagesFaustino 2008AbdelazizSeliemNo ratings yet
- Epidermodysplasia-Verruciformis YmjdDocument1 pageEpidermodysplasia-Verruciformis YmjdAndrés WunderwaldNo ratings yet
- Journal Reading TBDocument3 pagesJournal Reading TBnadia nanda salsabilaNo ratings yet
- Dermoskopi 2Document4 pagesDermoskopi 2Eldie RahimNo ratings yet
- Diagnosis of Tuberculosis Lancet 12Document1 pageDiagnosis of Tuberculosis Lancet 12OloyaNo ratings yet
- Diagnosis of Tuberculosis Lancet 13Document2 pagesDiagnosis of Tuberculosis Lancet 13OloyaNo ratings yet
- M: Elaine Crystine Vieira de Paiva Rua Pedro I, 1.033 Centro 60035-101 - Fortaleza - CE - BrazilDocument2 pagesM: Elaine Crystine Vieira de Paiva Rua Pedro I, 1.033 Centro 60035-101 - Fortaleza - CE - Brazilpruebaprueba321765No ratings yet
- Rak Nerki - Opis Przypadku U KoniaDocument4 pagesRak Nerki - Opis Przypadku U KoniaP KowalskiNo ratings yet
- Hallopeau 10.1001@jamadermatol.2019.3515Document1 pageHallopeau 10.1001@jamadermatol.2019.3515Faten HayderNo ratings yet
- Rapid Laboratory Diagnosis of Cholera in The Field 0035-9203 (89) 90733-5Document2 pagesRapid Laboratory Diagnosis of Cholera in The Field 0035-9203 (89) 90733-5JUAN HERNANDEZNo ratings yet
- IMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSDocument5 pagesIMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSjavelezhNo ratings yet
- Performance and Feasibility of Using Both Stool Culture and Nested PCR For Improved Detection of Typhoid Fever in Buea Health District, South West CameroonDocument9 pagesPerformance and Feasibility of Using Both Stool Culture and Nested PCR For Improved Detection of Typhoid Fever in Buea Health District, South West CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jogcr v1n2p0 enDocument3 pagesJogcr v1n2p0 enNabyl BektacheNo ratings yet
- Articulo Repro EquinaDocument4 pagesArticulo Repro EquinaKaren MoralesNo ratings yet
- Changing Pattern of Cutaneous Tuberculosis: A Prospective StudyDocument7 pagesChanging Pattern of Cutaneous Tuberculosis: A Prospective StudyErtyWitalayaL.ToruanNo ratings yet
- Jurnal Mikro-2Document8 pagesJurnal Mikro-2Mila KarmilaNo ratings yet
- Sanz 2004Document14 pagesSanz 2004subbumurugappan94No ratings yet
- Estudo Transversal HPV e Cancer - Lancet 1987Document4 pagesEstudo Transversal HPV e Cancer - Lancet 1987rafuxu22No ratings yet
- International Journal of LeprosyDocument2 pagesInternational Journal of LeprosyClaudia GilmanNo ratings yet
- Abstracts. Simpozion FMVT 2018Document17 pagesAbstracts. Simpozion FMVT 2018Iancu SebastianNo ratings yet
- Gonorrhoea in Men: Diagnostic Aspects and Changing Antibiotic Susceptibility PatternDocument4 pagesGonorrhoea in Men: Diagnostic Aspects and Changing Antibiotic Susceptibility PatternAlthaf FathanNo ratings yet
- Thesis Paper On PneumoniaDocument7 pagesThesis Paper On Pneumoniagbwwdfq5100% (1)
- Meningoencephalitis of Unknown Origin in Dogs CR - 881Document6 pagesMeningoencephalitis of Unknown Origin in Dogs CR - 881Ezequiel Davi Dos SantosNo ratings yet
- Canteros 2005Document6 pagesCanteros 2005Araceli EnríquezNo ratings yet
- Lettres A' La Re Daction / Gyne Cologie Obste Trique & Fertilite 43 (2015) 397-403 400Document3 pagesLettres A' La Re Daction / Gyne Cologie Obste Trique & Fertilite 43 (2015) 397-403 400terrydaNo ratings yet
- Nej Mo A 1515520Document10 pagesNej Mo A 1515520Franz RollerNo ratings yet
- Pathophysiology of Campylobacter Jejuni Infections of Humans 1999 Microbes and InfectionDocument11 pagesPathophysiology of Campylobacter Jejuni Infections of Humans 1999 Microbes and InfectionFrancisco GonzálezNo ratings yet
- Enhancing Immune Responses To Oral Vaccines StillDocument2 pagesEnhancing Immune Responses To Oral Vaccines StillSimbakutty VenkataramananNo ratings yet
- Daftar Pustaka No 6Document11 pagesDaftar Pustaka No 6Efti WeaslyNo ratings yet
- Fine 1986 Indicators of Periodontal Disease Activity An EvaluationDocument15 pagesFine 1986 Indicators of Periodontal Disease Activity An EvaluationBrenda Carolina Pattigno ForeroNo ratings yet
- DP Endo v01n3p017021 enDocument5 pagesDP Endo v01n3p017021 enasdfasdNo ratings yet
- KCP 1Document7 pagesKCP 1FurqanRidhaNo ratings yet
- IJBAIR232013Document5 pagesIJBAIR232013HUGO JOSUE MENDEZ GONZALEZNo ratings yet
- Answers To Continuing Medical Education QuestionsDocument2 pagesAnswers To Continuing Medical Education QuestionsKhalid AbdullahNo ratings yet
- Metastatic Intranasal Mastocytoma in A Dog CR - 892 - 30.JULDocument6 pagesMetastatic Intranasal Mastocytoma in A Dog CR - 892 - 30.JULEzequiel Davi Dos SantosNo ratings yet
- Whole Genome Analysis of Extensively Drug Resistant Mycobacterium Tuberculosis Strains in PeruDocument13 pagesWhole Genome Analysis of Extensively Drug Resistant Mycobacterium Tuberculosis Strains in PeruCarlos AscNo ratings yet
- Jurnal Kusta PDFDocument13 pagesJurnal Kusta PDFGustamas Indra Maulana100% (1)
- LCPG Diag Ex 9 Answers PDFDocument4 pagesLCPG Diag Ex 9 Answers PDFJulián Andres ArbelaezNo ratings yet
- XXXXXX 121Document11 pagesXXXXXX 121AndriantkNo ratings yet
- Resistencia de Uropatógenos en Infecciones de Tracto Urinario en Leon NicaraguaDocument4 pagesResistencia de Uropatógenos en Infecciones de Tracto Urinario en Leon NicaraguaMiguel AnguianoNo ratings yet
- Alisado Radicular de Cuadrante Versusalisado Radicular de Boca Completa en El Mismo DíaDocument8 pagesAlisado Radicular de Cuadrante Versusalisado Radicular de Boca Completa en El Mismo DíaNessa Barek VonMillerNo ratings yet
- Clinical Guidelines Secondary Prevention of Gastric CancerDocument1 pageClinical Guidelines Secondary Prevention of Gastric Cancerhenrique.uouNo ratings yet
- Idcases: Claudia Miranda, Michael A. Jaker, Valerie A. Fitzhugh-Kull, Lisa L. DeverDocument3 pagesIdcases: Claudia Miranda, Michael A. Jaker, Valerie A. Fitzhugh-Kull, Lisa L. Devercarlos barraganNo ratings yet
- Serologic Diagnosis of Tuberculosis Using A Simple Commercial Multiantigen AssayDocument6 pagesSerologic Diagnosis of Tuberculosis Using A Simple Commercial Multiantigen AssayTanveerNo ratings yet
- bmj00432 0066bDocument1 pagebmj00432 0066bNurintiNo ratings yet
- Prospectivo: Gov/Coronavirus/2019-Ncov/Prevent-Getting-Sick/Cloth-Face-Cover-Guidance - HTML Estatistics/Neiss-Injury-DataDocument2 pagesProspectivo: Gov/Coronavirus/2019-Ncov/Prevent-Getting-Sick/Cloth-Face-Cover-Guidance - HTML Estatistics/Neiss-Injury-DataLaira FogliarineNo ratings yet
- Serodiagnosis of Bartonella Bacilliformis Infection by Indirect Fluorescence Antibody Assay: Test Development and Application To A Population in An Area of Bartonellosis EndemicityDocument3 pagesSerodiagnosis of Bartonella Bacilliformis Infection by Indirect Fluorescence Antibody Assay: Test Development and Application To A Population in An Area of Bartonellosis EndemicitySOFIA ESTHER ROMERO MEDEROSNo ratings yet
- Paradental CystDocument2 pagesParadental CystAyoubNo ratings yet
- Microbial Pathogenesis: Short CommunicationDocument5 pagesMicrobial Pathogenesis: Short CommunicationPhuong ThaoNo ratings yet
- A Brief History of ProcalcitoninDocument2 pagesA Brief History of ProcalcitoninLeo LannyNo ratings yet
- Cell Movement and Neoplasia: Proceedings of the Annual Meeting of the Cell Tissue and Organ Culture Study Group, Held at the Janssen Research Foundation, Beerse, Belgium, May 1979From EverandCell Movement and Neoplasia: Proceedings of the Annual Meeting of the Cell Tissue and Organ Culture Study Group, Held at the Janssen Research Foundation, Beerse, Belgium, May 1979M. De BrabanderRating: 5 out of 5 stars5/5 (1)
- PRP ReviewDocument14 pagesPRP ReviewWei Sheng ChongNo ratings yet
- Kimura's Disease & ALHEDocument7 pagesKimura's Disease & ALHEWei Sheng ChongNo ratings yet
- pinpoint papular PMLEDocument4 pagespinpoint papular PMLEWei Sheng ChongNo ratings yet
- RCM in Bowen Disease Treated With PDTDocument6 pagesRCM in Bowen Disease Treated With PDTWei Sheng ChongNo ratings yet
- Etanercept in PsoriasisDocument5 pagesEtanercept in PsoriasisWei Sheng ChongNo ratings yet
- Paint PUVA in AADocument6 pagesPaint PUVA in AAWei Sheng ChongNo ratings yet
- NBUVB and Skin Cancer Incidence in Vitiligo PsoriasisDocument20 pagesNBUVB and Skin Cancer Incidence in Vitiligo PsoriasisWei Sheng ChongNo ratings yet
- Cubital Forearm Sign NTM InfectionDocument3 pagesCubital Forearm Sign NTM InfectionWei Sheng ChongNo ratings yet
- PCT Indurated Skin Iron OverloadDocument3 pagesPCT Indurated Skin Iron OverloadWei Sheng ChongNo ratings yet
- Omphalolith Surgical ExtractionDocument2 pagesOmphalolith Surgical ExtractionWei Sheng ChongNo ratings yet
- Biologics in Palmoplantar Psoriasis and Palmoplantar PustulosisDocument22 pagesBiologics in Palmoplantar Psoriasis and Palmoplantar PustulosisWei Sheng ChongNo ratings yet
- Cancer and ItchDocument6 pagesCancer and ItchWei Sheng ChongNo ratings yet
- Apremilast PI Europe Aug 2019Document14 pagesApremilast PI Europe Aug 2019Wei Sheng ChongNo ratings yet
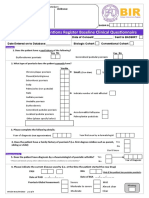
- BADBIR Registry Clinical Baseline Questionnaire v8 01.07.2015Document4 pagesBADBIR Registry Clinical Baseline Questionnaire v8 01.07.2015Wei Sheng ChongNo ratings yet
- Namibia Flipchart Algorithm Child Sep2010Document11 pagesNamibia Flipchart Algorithm Child Sep2010Gabriela Morante RuizNo ratings yet
- KSSM Bio F5 C2Document84 pagesKSSM Bio F5 C2Jia XuanNo ratings yet
- Envi. Sci-BuayaDocument1 pageEnvi. Sci-BuayaRochelle MaeNo ratings yet
- Lab 1. Understanding The Work of Microscopes: Campbell Biology, Reece Et Al, 2016) )Document7 pagesLab 1. Understanding The Work of Microscopes: Campbell Biology, Reece Et Al, 2016) )Ade Rizky FajrullohNo ratings yet
- OHAS Final Quiz 1 - Attempt ReviewDocument6 pagesOHAS Final Quiz 1 - Attempt ReviewNot Racist By The Way100% (1)
- An Elementary School Classroom in A Slum: Stanza 1Document2 pagesAn Elementary School Classroom in A Slum: Stanza 1Pooja RajeshNo ratings yet
- SIP Implementation Checklist Annex 2B - Child Protection PolicyDocument3 pagesSIP Implementation Checklist Annex 2B - Child Protection Policyfloren cuevasNo ratings yet
- Hardik Patel - Iciame2013 "RESEARCH PAPER-37"Document31 pagesHardik Patel - Iciame2013 "RESEARCH PAPER-37"hardik10888No ratings yet
- 01 Nov 07 AVAFCDProduct CodesDocument151 pages01 Nov 07 AVAFCDProduct CodesKo NgeNo ratings yet
- Engineering Change Notice (Field Change Notice) : ECN No. 2011-E-0119Document23 pagesEngineering Change Notice (Field Change Notice) : ECN No. 2011-E-0119Shabeer AhmadNo ratings yet
- ISAK 35 Non Profit Oriented EntitiesDocument48 pagesISAK 35 Non Profit Oriented Entitiesnabila dhiyaNo ratings yet
- Post Coital BleedingDocument8 pagesPost Coital BleedingMutiara SwNo ratings yet
- Expressing Apology: SMP Islam Nurus Sunnah SemarangDocument9 pagesExpressing Apology: SMP Islam Nurus Sunnah SemaranganggaNo ratings yet
- Quiz - No. - 2 Daily, Ma. Jhoan A.Document2 pagesQuiz - No. - 2 Daily, Ma. Jhoan A.Ma. Jhoan DailyNo ratings yet
- Product: WM 10 For Oil, Gas and Dual FuelDocument48 pagesProduct: WM 10 For Oil, Gas and Dual FuelHaqNo ratings yet
- Quality Inspectors - Job DescriptionDocument3 pagesQuality Inspectors - Job DescriptionMurugan.SubramaniNo ratings yet
- Unit 3 - Chocolate For BreakfastDocument14 pagesUnit 3 - Chocolate For BreakfastTrinhMy PhuongNo ratings yet
- Brochure - MS - WR - Plansifter Sirius - MPAK - EN - WEB - BID21Document8 pagesBrochure - MS - WR - Plansifter Sirius - MPAK - EN - WEB - BID21Lizandro ParedesNo ratings yet
- Republic of The Philippines Department of Education Region XIIDocument5 pagesRepublic of The Philippines Department of Education Region XIINethz Flores TresbeNo ratings yet
- CRF For HypertensionDocument10 pagesCRF For HypertensionManishkumar K SinghNo ratings yet
- Risk Table JF 25 MarchDocument1 pageRisk Table JF 25 MarchPrestoneKNo ratings yet
- 20b GT PART2 PDFDocument178 pages20b GT PART2 PDFHANIF AKBARNo ratings yet
- RD Manual 02250201-297 R01 EnglishDocument146 pagesRD Manual 02250201-297 R01 EnglishTravis HamelNo ratings yet
- Vibration Shock MountsDocument20 pagesVibration Shock MountsmNo ratings yet
- Lecturas Ingles Saber Pro 2019Document13 pagesLecturas Ingles Saber Pro 2019Wilson OspinoNo ratings yet
- ZIM ART Guidelines 2016 - Review FinalDocument136 pagesZIM ART Guidelines 2016 - Review FinalCollen LihakaNo ratings yet
- MGTC Annual Report 2021Document188 pagesMGTC Annual Report 2021Jenny AbdullahNo ratings yet
- Seattle Children's - 2009 Community Benefit ReportDocument32 pagesSeattle Children's - 2009 Community Benefit ReportJeneen CoydanNo ratings yet
- Magnetic Properties of Co Ordination CompoundsDocument14 pagesMagnetic Properties of Co Ordination CompoundsbnkjayaNo ratings yet
- 4 Intelligence Vs Non-IntelligenceDocument28 pages4 Intelligence Vs Non-IntelligenceSani BlackNo ratings yet