You might also like
- (Early Modern History - Society and Culture) Laura J. McGough (Auth.) - Gender, Sexuality, and Syphilis in Early Modern Venice - The Disease That Came To Stay-Palgrave Macmillan UK (2010) - 4 PDFDocument213 pages(Early Modern History - Society and Culture) Laura J. McGough (Auth.) - Gender, Sexuality, and Syphilis in Early Modern Venice - The Disease That Came To Stay-Palgrave Macmillan UK (2010) - 4 PDFMarianaNo ratings yet
- Tobacco Cessation PlanDocument11 pagesTobacco Cessation PlanEsteban García EcheverryNo ratings yet
- Surgical ConsentDocument2 pagesSurgical ConsentTeanu Jose Gabrillo TamayoNo ratings yet
- Notice of Privacy Practices Revised 11Document2 pagesNotice of Privacy Practices Revised 11api-279009912No ratings yet
- Patients Bill of RightsDocument13 pagesPatients Bill of RightsJason ArzagaNo ratings yet
- Informed Consent For Laparoscopic CholecystectomyDocument5 pagesInformed Consent For Laparoscopic CholecystectomyJatrik BiswasNo ratings yet
- General Consent Form English 29-IV-09Document3 pagesGeneral Consent Form English 29-IV-09rubenguzNo ratings yet
- Physician Observer Application: Information/documentation To Be Included With Your Completed ApplicationDocument15 pagesPhysician Observer Application: Information/documentation To Be Included With Your Completed ApplicationCarlos Del Carpio EnriquezNo ratings yet
- Medical Record General Admission ConsentDocument1 pageMedical Record General Admission ConsentMohammedNo ratings yet
- Mama Nov 10, 2022Document1 pageMama Nov 10, 2022Little DreamcatcherNo ratings yet
- Clinical Observership Application Clinical NutritionDocument4 pagesClinical Observership Application Clinical Nutritionkhalidbushra635No ratings yet
- HIPAA InformationDocument1 pageHIPAA InformationFOOTANKLEPSLNo ratings yet
- QR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Document1 pageQR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Yel BNo ratings yet
- Chapter 15 Legal Aspects and The Nurse Part 2Document10 pagesChapter 15 Legal Aspects and The Nurse Part 2Nancy Jane TaguilingNo ratings yet
- Judicial Claims ClauseDocument2 pagesJudicial Claims ClauserubenguzNo ratings yet
- Data Privacy Consent: II. Consent For Procedure(s)Document1 pageData Privacy Consent: II. Consent For Procedure(s)kNo ratings yet
- All FormsDocument13 pagesAll FormsSam EmekaNo ratings yet
- Authorization Form: (Please Check All Applicable Boxes)Document3 pagesAuthorization Form: (Please Check All Applicable Boxes)Apostle Verbenia SousaNo ratings yet
- Consent, Confidentiality and ResponsibilitiesDocument2 pagesConsent, Confidentiality and ResponsibilitieserenealNo ratings yet
- FACILITY NAME: - : I. Consent To Surgery or Special ProcedureDocument11 pagesFACILITY NAME: - : I. Consent To Surgery or Special ProcedureJack Tedesco0% (1)
- HIPAA Patient Authorization For ROI FormDocument1 pageHIPAA Patient Authorization For ROI FormDawn M. Rapoport, Rapoport Law GroupNo ratings yet
- Patients' Rights: Online CourseDocument16 pagesPatients' Rights: Online CoursegopscharanNo ratings yet
- Dianakleine Job37 Policy4Document1 pageDianakleine Job37 Policy4api-535145429No ratings yet
- HEALTH CARE POWER OF ATTORNEY (SC Statutory Form)Document7 pagesHEALTH CARE POWER OF ATTORNEY (SC Statutory Form)Alexandria Broughton SkinnerNo ratings yet
- Contoh General ConsentDocument1 pageContoh General ConsentMahendra AbdythamaNo ratings yet
- Nevada Living WillDocument7 pagesNevada Living WillRocketLawyer100% (1)
- Medical ReleaseDocument2 pagesMedical ReleasekhangpngNo ratings yet
- Ncad WillDocument12 pagesNcad Willoatmealchocolate79100% (1)
- Please Read The Entire Form Carefully Before SigningDocument2 pagesPlease Read The Entire Form Carefully Before SigningKoh LudzNo ratings yet
- Patient Rights and ResponsibilitiesDocument8 pagesPatient Rights and ResponsibilitiesIwan BudhihartoNo ratings yet
- 01-RCD General Consent Form For TreatmentDocument2 pages01-RCD General Consent Form For TreatmentSaad HussainNo ratings yet
- Recredentialing Packet 2010 FinalDocument3 pagesRecredentialing Packet 2010 Finaljanita hartanto100% (1)
- Consent Ergonomic Assessment FillableDocument2 pagesConsent Ergonomic Assessment FillableJess McDonaldNo ratings yet
- Medical Transfer Consent FormDocument2 pagesMedical Transfer Consent Formqwertyuiopkmrr100% (1)
- Medical SurgicalDocument13 pagesMedical SurgicalKrzia TehNo ratings yet
- Healthcare Professional AgreementDocument7 pagesHealthcare Professional Agreementnavneetshekhar.11No ratings yet
- Notice of Privacy PracticesDocument6 pagesNotice of Privacy PracticesJames LanierNo ratings yet
- J. Bruce Bayne HIPPA FormDocument5 pagesJ. Bruce Bayne HIPPA FormWilliam BayneNo ratings yet
- Años - Nda Student Affiliate Trainee Faculty Clinical InstructorDocument2 pagesAños - Nda Student Affiliate Trainee Faculty Clinical InstructorSimon KunNo ratings yet
- Healthy LIC - Patient CONSENT Form EnglishDocument4 pagesHealthy LIC - Patient CONSENT Form EnglishTheFloatingHospitalNo ratings yet
- Congvax Consent FormDocument3 pagesCongvax Consent FormRico MaligayaNo ratings yet
- 9Authorization-to-Release-Medical-Records-to-Third-Party-HIPAA (1) (1)Document1 page9Authorization-to-Release-Medical-Records-to-Third-Party-HIPAA (1) (1)jenn79562No ratings yet
- Dpo Ah C Louie Wayne PittmanDocument9 pagesDpo Ah C Louie Wayne PittmanCricketandScott HintonNo ratings yet
- BHJ Online Consent 2021Document3 pagesBHJ Online Consent 2021Sherryl SarmientoNo ratings yet
- Notice of Privacy PracticesDocument3 pagesNotice of Privacy PracticesAngel AbstonNo ratings yet
- General Admission ConsentDocument2 pagesGeneral Admission ConsentPratiksha SinghNo ratings yet
- Consent and Confedentiality, Conflict - 2nd LectureDocument39 pagesConsent and Confedentiality, Conflict - 2nd Lectureaymanbassyouni77No ratings yet
- YL Camping Consent and Health FormDocument4 pagesYL Camping Consent and Health Formmcronin1970No ratings yet
- C&a Consent FormsDocument28 pagesC&a Consent Formsjgcj477rh9No ratings yet
- 2011 Religious Exemption Request Form 081211Document1 page2011 Religious Exemption Request Form 081211mtaivalmaaNo ratings yet
- Nebraska Living WillDocument4 pagesNebraska Living WillRocketLawyerNo ratings yet
- Informed ConsentDocument4 pagesInformed ConsentRaja EllysyaNo ratings yet
- Patient Waiver of LiabilityDocument1 pagePatient Waiver of LiabilityGlendaNo ratings yet
- Advocare Consent Disclosure Authorization PDFDocument2 pagesAdvocare Consent Disclosure Authorization PDFAsnaifa Bint MamintalNo ratings yet
- Advanced Directive & Durable Power of Attorney For Health CareDocument6 pagesAdvanced Directive & Durable Power of Attorney For Health CareTexieraNo ratings yet
- HO Legality of Patient EducationDocument3 pagesHO Legality of Patient EducationNOEL YRIGONNo ratings yet
- Steps Forward Hipaa Privacy FormsDocument26 pagesSteps Forward Hipaa Privacy FormsdawnNo ratings yet
- Filipino Patient'S Bill of Rights: Banagen, Philip BDocument3 pagesFilipino Patient'S Bill of Rights: Banagen, Philip BLegendXNo ratings yet
- PT Agreement IIDocument1 pagePT Agreement IIapi-301624030No ratings yet
- HIPAA Notice of Privacy PracticesDocument5 pagesHIPAA Notice of Privacy PracticesJennifer SchwartzNo ratings yet
- Form 7A - Grant of Leave To Involuntary Inpatient: Sections: 105Document2 pagesForm 7A - Grant of Leave To Involuntary Inpatient: Sections: 105prabhaNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Week 3 - AssignmentDocument4 pagesWeek 3 - AssignmentEsteban García EcheverryNo ratings yet
- WK7 Assgn GrantDocument11 pagesWK7 Assgn GrantEsteban García EcheverryNo ratings yet
- 0Document8 pages0Esteban García EcheverryNo ratings yet
- NURS-FPX4020 - JohanneDesiree - Assessment1-1Document7 pagesNURS-FPX4020 - JohanneDesiree - Assessment1-1Esteban García EcheverryNo ratings yet
- twUiK7v2pXHeplQJ 0Document6 pagestwUiK7v2pXHeplQJ 0Esteban García EcheverryNo ratings yet
- WK3 Assgn Leconte LDocument8 pagesWK3 Assgn Leconte LEsteban García EcheverryNo ratings yet
- CF Rca TemplateDocument8 pagesCF Rca TemplateEsteban García EcheverryNo ratings yet
- OIGHHS Federal ComplianceDocument19 pagesOIGHHS Federal ComplianceEsteban García EcheverryNo ratings yet
- Do Not Resuscitate in The Operating Room - Suspend or Not To SuspendDocument4 pagesDo Not Resuscitate in The Operating Room - Suspend or Not To SuspendEsteban García EcheverryNo ratings yet
- Lesotho Public Health Sector Expenditure Review - 2017Document91 pagesLesotho Public Health Sector Expenditure Review - 2017Esteban García EcheverryNo ratings yet
- 11 Malbasic Rey PosaricDocument20 pages11 Malbasic Rey PosaricEsteban García EcheverryNo ratings yet
- Making SMART Goals Smarter: in This ArticleDocument5 pagesMaking SMART Goals Smarter: in This ArticleEsteban García EcheverryNo ratings yet
- Prevalence of Workplace Physical Violence Against Health Care Professionals by Patients and Visitors: A Systematic Review and Meta-AnalysisDocument19 pagesPrevalence of Workplace Physical Violence Against Health Care Professionals by Patients and Visitors: A Systematic Review and Meta-AnalysisEsteban García EcheverryNo ratings yet
- 2020 Annual Compliance Update-Core - Clinical For WebDocument30 pages2020 Annual Compliance Update-Core - Clinical For WebEsteban García EcheverryNo ratings yet
- 2020 Annual Compliance Update-Core - Clinical For WebDocument30 pages2020 Annual Compliance Update-Core - Clinical For WebEsteban García EcheverryNo ratings yet
- Case Study Week 3 AssignmentDocument2 pagesCase Study Week 3 AssignmentEsteban García EcheverryNo ratings yet
- Foodborne Illness Outbreak QuestionnaireDocument1 pageFoodborne Illness Outbreak QuestionnaireEsteban García EcheverryNo ratings yet
- Comparing Hinduism and Jainism World Religions University of Bridgeport Mariah Y. ArringtonDocument3 pagesComparing Hinduism and Jainism World Religions University of Bridgeport Mariah Y. ArringtonEsteban García EcheverryNo ratings yet
- Personal Continuous Quality Improvement Project EvaulationDocument2 pagesPersonal Continuous Quality Improvement Project EvaulationEsteban García EcheverryNo ratings yet
- Comparing and Contrasting The Four Yoga Styles in Hinduism Rakeshia Gregory WREL216: Philosophy of World Religions Dr. Caicco April 2, 2021Document4 pagesComparing and Contrasting The Four Yoga Styles in Hinduism Rakeshia Gregory WREL216: Philosophy of World Religions Dr. Caicco April 2, 2021Esteban García EcheverryNo ratings yet
- Running Head: Comprehensive Healt History and Genogram Assignment 1Document10 pagesRunning Head: Comprehensive Healt History and Genogram Assignment 1Esteban García EcheverryNo ratings yet
- HA 535 - Assignment Two Instruction - Coding Sheet Summary Table ExampleDocument2 pagesHA 535 - Assignment Two Instruction - Coding Sheet Summary Table ExampleEsteban García EcheverryNo ratings yet
- Ethiopia School Health Program Framework August 2017 - FINALDocument118 pagesEthiopia School Health Program Framework August 2017 - FINALKeneniNo ratings yet
- Agha Khan UniversityDocument8 pagesAgha Khan UniversityFawadNo ratings yet
- Topik 14. Word Association Medical VocabularyDocument4 pagesTopik 14. Word Association Medical VocabularyioakasNo ratings yet
- Volume I C3 TheWatershedYears1828 1830Document46 pagesVolume I C3 TheWatershedYears1828 1830Ramesh Bhagwani100% (2)
- Vocabulary Files c1 Unit 13Document22 pagesVocabulary Files c1 Unit 13Viet ThangNo ratings yet
- Class 8 Chapter 2 With AnswersDocument11 pagesClass 8 Chapter 2 With AnswersAsma MerchantNo ratings yet
- Infection Control Guidelines: Ahmed AnwarDocument73 pagesInfection Control Guidelines: Ahmed AnwarHosam GomaaNo ratings yet
- Revision For The Mid-Term Test - Grade 2Document4 pagesRevision For The Mid-Term Test - Grade 2LinhLyNo ratings yet
- HepatitisBThesis Somaliland Somalia SanaagDocument67 pagesHepatitisBThesis Somaliland Somalia SanaagAhmed Osman sh: mahamedNo ratings yet
- Reflection: "See The Light at The End of The Tunnel"Document2 pagesReflection: "See The Light at The End of The Tunnel"John Flex SingculanNo ratings yet
- Department of Health - Emerging and Re-Emerging Infectious Disease Program - 2011-10-17Document3 pagesDepartment of Health - Emerging and Re-Emerging Infectious Disease Program - 2011-10-17John Oliver Y. MatuguinaNo ratings yet
- CHN Battexam 1Document25 pagesCHN Battexam 1jimwelluismagno27No ratings yet
- At The Doctor - Multiple ChoiceDocument10 pagesAt The Doctor - Multiple ChoiceGinaNo ratings yet
- Incovacc Fact SheetDocument1 pageIncovacc Fact SheetSai SapNo ratings yet
- Early Warning Alert and Response in Emergencies: An Operational GuideDocument208 pagesEarly Warning Alert and Response in Emergencies: An Operational GuideVitaNo ratings yet
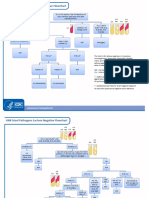
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Urinary Tract Infection in ChildrenDocument45 pagesUrinary Tract Infection in ChildrenMuhammad HaziqNo ratings yet
- Antibiotics Simplified 1st Edition DR - Osama Ma3rofDocument57 pagesAntibiotics Simplified 1st Edition DR - Osama Ma3rofDark AngelNo ratings yet
- Epstein-Barr Virus Laboratory Testing - CDCDocument1 pageEpstein-Barr Virus Laboratory Testing - CDCKonstantinidis LeonidasNo ratings yet
- IELTS A - R - W Collocations Handout 3Document2 pagesIELTS A - R - W Collocations Handout 3Lịch PhạmNo ratings yet
- Official Food-Safety Neogen-Culture-Media Catalog En-UsDocument84 pagesOfficial Food-Safety Neogen-Culture-Media Catalog En-UsRudresh UjjaNo ratings yet
- CHAPTER 2 Literature ReviewDocument6 pagesCHAPTER 2 Literature ReviewSibanda MqondisiNo ratings yet
- Mask WearingDocument2 pagesMask WearingNghi PhuongNo ratings yet
- Microbial EcologyDocument49 pagesMicrobial EcologyWahab KhaniNo ratings yet
- Mary MallonDocument4 pagesMary MallonChristelle MalaitNo ratings yet
- Chapter 3Document9 pagesChapter 3agelesswap100% (1)
- Rabies VaccinesDocument2 pagesRabies VaccinesmadebagussnNo ratings yet
- Assignment: Btec FPTDocument23 pagesAssignment: Btec FPTĐinh Khải TuệNo ratings yet