You might also like
- Psych CardsDocument10 pagesPsych CardsJennifer Rodriguez96% (24)
- Psychopharmacology 2 AntidepressantsDocument7 pagesPsychopharmacology 2 AntidepressantsBea Samonte100% (2)
- Current Clinical Strategies Psychiatry - Rhoda K HahnDocument125 pagesCurrent Clinical Strategies Psychiatry - Rhoda K HahnLetitia Claudia DobraniciNo ratings yet
- PSE10 MS056 - Present - State - ExaminationDocument18 pagesPSE10 MS056 - Present - State - ExaminationFrancisco Javier Salazar Núñez100% (1)
- StahleDocument12 pagesStahlekhaledazima0% (2)
- Decisive Chip Heath and Dan HeathDocument1 pageDecisive Chip Heath and Dan HeathHoratiu BahneanNo ratings yet
- Sample Complaint For Foreclosure of Mechanics Lien in CaliforniaDocument3 pagesSample Complaint For Foreclosure of Mechanics Lien in CaliforniacellajonesNo ratings yet
- K P Differential Diagnosis Pyramid: OPMAPS: Sychiatry EvisionDocument36 pagesK P Differential Diagnosis Pyramid: OPMAPS: Sychiatry EvisionArama CristiNo ratings yet
- DELIRIUM PresentationDocument26 pagesDELIRIUM PresentationAnkush Sharma100% (1)
- Biological Treatments in PsychiatryDocument56 pagesBiological Treatments in PsychiatryNurul AfzaNo ratings yet
- 10 Cognitive DisordersDocument16 pages10 Cognitive DisordersFarrah MaeNo ratings yet
- PSYCHIATRY Course NotesDocument43 pagesPSYCHIATRY Course NotesNisha PillaiNo ratings yet
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 pagesShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenNo ratings yet
- Module 3 - D - Antipsychotics For Bipolar DisorderDocument19 pagesModule 3 - D - Antipsychotics For Bipolar Disorderpsychopharmacology100% (2)
- DSM-IV Criteria MnemonicsDocument4 pagesDSM-IV Criteria Mnemonicsleonyap100% (1)
- Introduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPDocument33 pagesIntroduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPSachiko Yosores100% (1)
- Psych Ch. 5 NotesDocument7 pagesPsych Ch. 5 NotesHaylle ThomasNo ratings yet
- AntipsychoticsDocument22 pagesAntipsychoticsvinodksahuNo ratings yet
- Geriatric Giants - DR SeymourDocument108 pagesGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Psychiatry CasesDocument65 pagesPsychiatry CasesakeelNo ratings yet
- Varun Kumar, 2017 - Getting Started in PsychiatryDocument148 pagesVarun Kumar, 2017 - Getting Started in PsychiatryBernard FZ100% (1)
- "Serotonin Syndrome Causes HARM": Psychiatry PharamacologyDocument9 pages"Serotonin Syndrome Causes HARM": Psychiatry Pharamacologytycobb63100% (4)
- Psychiatry: Mental State ExaminationDocument3 pagesPsychiatry: Mental State ExaminationSok-Moi Chok100% (3)
- PsychDocument12 pagesPsychkaranNo ratings yet
- Drugs For Psyciatric DisordersDocument19 pagesDrugs For Psyciatric Disordersapi-36993610% (1)
- Treatment Modalities For Mood DisordersDocument55 pagesTreatment Modalities For Mood DisordersGlory MimiNo ratings yet
- Psychiatry Made EasyDocument14 pagesPsychiatry Made EasyTinesh Rajah83% (6)
- Psych History Format 2017Document2 pagesPsych History Format 2017Anne SisonNo ratings yet
- Antipsychotics HandoutDocument25 pagesAntipsychotics HandoutTeddy Kurniady ThaherNo ratings yet
- AntidepressantsDocument5 pagesAntidepressantsUm HamoOd100% (2)
- Glossary of Psychiatric TerminologyDocument20 pagesGlossary of Psychiatric Terminologyphoebe_62002239No ratings yet
- AntipsychoticsDocument10 pagesAntipsychoticswawing16No ratings yet
- PsychiatryDocument92 pagesPsychiatrykimNo ratings yet
- Pharmacology - (5) Psychotic DrugsDocument8 pagesPharmacology - (5) Psychotic DrugsSamantha DiegoNo ratings yet
- Psychiatric Disorder.Document127 pagesPsychiatric Disorder.Minlik-alew DejenieNo ratings yet
- Psych Ch. 7 Notes (Tutor)Document5 pagesPsych Ch. 7 Notes (Tutor)Haylle ThomasNo ratings yet
- Sudden Onset (Within 2 Weeks) of at Least One of TheDocument2 pagesSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaNo ratings yet
- Antidepressant DrugsDocument21 pagesAntidepressant DrugsKashis SharmaNo ratings yet
- Practical Notebook Adult PsychiatryDocument121 pagesPractical Notebook Adult PsychiatryCarly DyaNo ratings yet
- 4.2 Psychotropic Drugs Used in PsychiatryDocument32 pages4.2 Psychotropic Drugs Used in PsychiatryAmar Nur Arif ZazuliNo ratings yet
- Glossary of Psychiatric TermsDocument42 pagesGlossary of Psychiatric TermsÏtz ShãrîNo ratings yet
- PMHNP Case Study - EditedDocument7 pagesPMHNP Case Study - EditedSoumyadeep BoseNo ratings yet
- Psych DrugsDocument3 pagesPsych DrugsSwarna BanikNo ratings yet
- Pharmacotherapy in PschiatryDocument8 pagesPharmacotherapy in PschiatryygfhdgNo ratings yet
- Translate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeDocument76 pagesTranslate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeHadi GunaNo ratings yet
- Mental Health and Psychiatric Nursing: Vernalin B. Terrado, RNDocument35 pagesMental Health and Psychiatric Nursing: Vernalin B. Terrado, RNverna100% (1)
- Clerkship - Psychiatric History and MseDocument24 pagesClerkship - Psychiatric History and MsefahmiNo ratings yet
- Laboratory Tests and Imaging in PsychiatryDocument29 pagesLaboratory Tests and Imaging in Psychiatrypainpainlan100% (1)
- DeliriumDocument2 pagesDeliriumAngelique van Tonder100% (2)
- A) A/E of Moclobemide SNATCH: A) Pharmacology 1) Anti-DepressantsDocument10 pagesA) A/E of Moclobemide SNATCH: A) Pharmacology 1) Anti-DepressantsNur Atiqah Mohd AzliNo ratings yet
- Psychiatry Notes - Depressive DisorderDocument2 pagesPsychiatry Notes - Depressive DisorderLiSenNo ratings yet
- USMLE Mnemonics PsychDocument4 pagesUSMLE Mnemonics Psychzhzizhzi100% (3)
- Study Psych DrugsDocument14 pagesStudy Psych Drugsapi-369732698% (47)
- Study Guide Test 1Document11 pagesStudy Guide Test 1jwasylow13No ratings yet
- Provisional: Borderline Personality Disorder Differential DXDocument6 pagesProvisional: Borderline Personality Disorder Differential DXhernandez2812No ratings yet
- Brain, Behavior & PsychopharmacologyDocument42 pagesBrain, Behavior & PsychopharmacologyRichky Nurhakim100% (4)
- Neuroleptics & AnxiolyticsDocument65 pagesNeuroleptics & AnxiolyticsAntonPurpurovNo ratings yet
- Notes On Psychiatry: TypesDocument17 pagesNotes On Psychiatry: TypesMAY100% (1)
- Terms in The Field of PsychiatryDocument18 pagesTerms in The Field of PsychiatryOchie YecyecanNo ratings yet
- Progress in Neurology and Psychiatry: An Annual ReviewFrom EverandProgress in Neurology and Psychiatry: An Annual ReviewE. A. SpiegelNo ratings yet
- (Labor 2 - Atty. Nolasco) : G.R. No. 196539 Perez, J. Digest By: IntiaDocument2 pages(Labor 2 - Atty. Nolasco) : G.R. No. 196539 Perez, J. Digest By: IntiaRaymund CallejaNo ratings yet
- Harm ReductionDocument2 pagesHarm ReductionDarren CariñoNo ratings yet
- Homeopathic Materia Medica Vol 1Document259 pagesHomeopathic Materia Medica Vol 1LotusGuy Hans100% (3)
- SpecPro Rule 77Document13 pagesSpecPro Rule 77angelescrishanneNo ratings yet
- Work ImmersionDocument11 pagesWork ImmersionSherwin Jay BentazarNo ratings yet
- Mary ToostealDocument4 pagesMary ToostealtesttestNo ratings yet
- Sponsorship AgreementDocument2 pagesSponsorship Agreementprakhar singhNo ratings yet
- GR Nos. 103501-03 and 103507: Tabuena Vs SandiganbayanDocument30 pagesGR Nos. 103501-03 and 103507: Tabuena Vs SandiganbayanteepeeNo ratings yet
- 6843 21205 1 PBDocument8 pages6843 21205 1 PBikc711No ratings yet
- Making A Reaction StatementDocument6 pagesMaking A Reaction StatementKharisma AnastasisNo ratings yet
- Kohlberg 29Document32 pagesKohlberg 29wendy nguNo ratings yet
- M019 A Ylshyn-TiliDocument4 pagesM019 A Ylshyn-TiliTolkynNo ratings yet
- State - CIF - Parent - Handbook - I - Understanding - Transfer - Elgibility - August - 2021-11 (Dragged) PDFDocument1 pageState - CIF - Parent - Handbook - I - Understanding - Transfer - Elgibility - August - 2021-11 (Dragged) PDFDaved BenefieldNo ratings yet
- Philosophy 200: Ethics: Pursue AvoidDocument9 pagesPhilosophy 200: Ethics: Pursue AvoidAngela Del CastilloNo ratings yet
- Sayson TheStruggleAgainstMining-PAD2004Document106 pagesSayson TheStruggleAgainstMining-PAD2004junsaturayNo ratings yet
- Political Order in Changing SocietiesDocument83 pagesPolitical Order in Changing SocietiesMichiru2011100% (1)
- The Relationship Between Residential Satisfaction Sense of CommuDocument373 pagesThe Relationship Between Residential Satisfaction Sense of CommuKhalid Ali Saif Al-ShamsiNo ratings yet
- No HomeworkDocument2 pagesNo HomeworkRhea Somollo BolatinNo ratings yet
- XI-Poem 1 Ms AmmaraDocument10 pagesXI-Poem 1 Ms AmmaraAmmara KhalidNo ratings yet
- Mental Health Nursing Assignment Sample: WWW - Newessays.co - UkDocument15 pagesMental Health Nursing Assignment Sample: WWW - Newessays.co - UkAriadne MangondatoNo ratings yet
- Death Certificate FormDocument3 pagesDeath Certificate FormMumtahina ZimeenNo ratings yet
- Further White Estate Lawsuit Negotiation CorrespondenceDocument16 pagesFurther White Estate Lawsuit Negotiation CorrespondenceDanielBabylone100% (1)
- Lesson 1: The Human Person, Image of GodDocument8 pagesLesson 1: The Human Person, Image of GodJhon Gabriel DelacruzNo ratings yet
- T7 B12 Flight 93 Calls - Todd Beamer FDR - 2 FBI 302s Re NK 5381 - Lead Control Number 417Document3 pagesT7 B12 Flight 93 Calls - Todd Beamer FDR - 2 FBI 302s Re NK 5381 - Lead Control Number 4179/11 Document ArchiveNo ratings yet
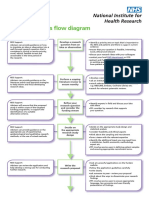
- Research Process Flow Chart A4 WebDocument2 pagesResearch Process Flow Chart A4 WebEma FatimahNo ratings yet
- Dantes Inferno - 9 Circles of HellDocument23 pagesDantes Inferno - 9 Circles of Hellapi-305331060No ratings yet
- Siti Atiqah Binti Mohd Sidin A30109190004 Ess222Document10 pagesSiti Atiqah Binti Mohd Sidin A30109190004 Ess222Mohd Zulhelmi Idrus100% (1)
- Philo12 q1 w1-2 APILDocument27 pagesPhilo12 q1 w1-2 APILJoiemmy GayudanNo ratings yet