You might also like
- Fungi52 52.9537Document6 pagesFungi52 52.9537Reza PutradinataNo ratings yet
- Pediatric Round PneumoniaDocument4 pagesPediatric Round PneumoniaSalwa Zahra TsamaraNo ratings yet
- A Rare Cause of Endocarditis: Streptococcus PyogenesDocument3 pagesA Rare Cause of Endocarditis: Streptococcus PyogenesYusuf BrilliantNo ratings yet
- Pulmonary Miliary Tuberculosis Complicated With Tuberculous Spondylitis An Extraordinary Rare Association: A Case ReportDocument5 pagesPulmonary Miliary Tuberculosis Complicated With Tuberculous Spondylitis An Extraordinary Rare Association: A Case ReportIsmail Eko SaputraNo ratings yet
- Jurnal Bronchitis Dengan AsmaDocument5 pagesJurnal Bronchitis Dengan AsmaMauLan SaputraNo ratings yet
- F - CMCRep 1 Assy Et Al - 1405Document2 pagesF - CMCRep 1 Assy Et Al - 1405faegrerh5ju75yu34yNo ratings yet
- Case Report: A 75-Year-Old Female With Hemoptysis and Recurrent Respiratory InfectionsDocument4 pagesCase Report: A 75-Year-Old Female With Hemoptysis and Recurrent Respiratory InfectionsIRa SyalalaNo ratings yet
- Necrotizing Pneumonitis Caused by Mycoplasma Pneumoniae in Pediatric PatientsDocument4 pagesNecrotizing Pneumonitis Caused by Mycoplasma Pneumoniae in Pediatric Patientswawa chenNo ratings yet
- 500 FullDocument4 pages500 FullAina NurlailaNo ratings yet
- Case Report: Systemic Steroid Treatment For Severe Expanding Pneumococcal PneumoniaDocument4 pagesCase Report: Systemic Steroid Treatment For Severe Expanding Pneumococcal PneumoniaadhiniNo ratings yet
- Pathophysiological Study of Chronic Necrotizing Pulmonary AspergillosisDocument5 pagesPathophysiological Study of Chronic Necrotizing Pulmonary AspergillosisSyaiful IslamNo ratings yet
- Recurrent Pneumonia Caused by Rare Granular Cell TumorDocument7 pagesRecurrent Pneumonia Caused by Rare Granular Cell TumorJoshua MendozaNo ratings yet
- Empyema Thoracis Caused by Drug-Resistant S. aureusDocument6 pagesEmpyema Thoracis Caused by Drug-Resistant S. aureuspqrsehunNo ratings yet
- Bronchitis Obliterans Due To Mycoplasma PneumoniaDocument7 pagesBronchitis Obliterans Due To Mycoplasma Pneumoniawawa chenNo ratings yet
- A Case of Pulmonary Aspergilloma and ActinomycosisDocument4 pagesA Case of Pulmonary Aspergilloma and ActinomycosisNova PurbaNo ratings yet
- Chronic Pulmonary Aspergillosis in A Patient With hyper-IgE SyndromeDocument3 pagesChronic Pulmonary Aspergillosis in A Patient With hyper-IgE SyndromeWalid AissaNo ratings yet
- Stevens-Johnson Syndrome Without Skin Lesions: Case ReportDocument4 pagesStevens-Johnson Syndrome Without Skin Lesions: Case ReportYona LadyventiniNo ratings yet
- Epiglotitis DCHDocument6 pagesEpiglotitis DCHLu BfNo ratings yet
- Pulmonary Tuberculosis Presenting with ARDSDocument5 pagesPulmonary Tuberculosis Presenting with ARDSCimol AgustinaNo ratings yet
- Pulmonary Interstitial Emphysema Complicating Pneumonia in An Unventilated Term InfantDocument3 pagesPulmonary Interstitial Emphysema Complicating Pneumonia in An Unventilated Term Infantindra_poetoetNo ratings yet
- Case Report Proteus Species Infection: A Diagnostic DilemmaDocument5 pagesCase Report Proteus Species Infection: A Diagnostic DilemmaTengku AdriansyahNo ratings yet
- Jurnal 7 BronkiolitisDocument7 pagesJurnal 7 BronkiolitisIrsanti sasmitaNo ratings yet
- Paediatric Empyema: A Case Report and Literature ReviewDocument5 pagesPaediatric Empyema: A Case Report and Literature ReviewphobicmdNo ratings yet
- Rhizomucor Scedosporium: Case ReportDocument6 pagesRhizomucor Scedosporium: Case ReportPaul ColburnNo ratings yet
- Early Diagnosis of Kartagener's SyndromeDocument8 pagesEarly Diagnosis of Kartagener's SyndromeHendra SusantoNo ratings yet
- Lesoes Cisticas HIVDocument5 pagesLesoes Cisticas HIVAndrey Barbosa PimentaNo ratings yet
- Eosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportDocument5 pagesEosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportSabrina JonesNo ratings yet
- Mediastinal Tuberculous Lymphadenitis Presenting With Insidious Back Pain in A Male Adult: A Case Report and Review of The LiteratureDocument7 pagesMediastinal Tuberculous Lymphadenitis Presenting With Insidious Back Pain in A Male Adult: A Case Report and Review of The Literaturez9tpwgb5nwNo ratings yet
- The Role of High-Resolution Chest CT in The Diagnosis of Neuroendocrine Cell Hyperplasia of Infancy - A Rare Form of Pediatric Interstitial Lung DiseaseDocument3 pagesThe Role of High-Resolution Chest CT in The Diagnosis of Neuroendocrine Cell Hyperplasia of Infancy - A Rare Form of Pediatric Interstitial Lung DiseaseWalid AissaNo ratings yet
- Case ARDSDocument16 pagesCase ARDSAida SiregarNo ratings yet
- Computed Tomography Findings of Community-Acquired Immunocompetent Patient: A Case ReportDocument4 pagesComputed Tomography Findings of Community-Acquired Immunocompetent Patient: A Case ReportDenta HaritsaNo ratings yet
- Case Report: Hydropneumothorax in Children: A Rare Complication of A Bacterial PneumoniaDocument5 pagesCase Report: Hydropneumothorax in Children: A Rare Complication of A Bacterial PneumoniaNadya NovianiNo ratings yet
- Pulmonary Histoplasmosis Halo Sign CTDocument2 pagesPulmonary Histoplasmosis Halo Sign CTSharom R. AlvarezNo ratings yet
- A 7-Year-Old Girl With Dyspnea and Rash: AnswertophotoquizDocument2 pagesA 7-Year-Old Girl With Dyspnea and Rash: AnswertophotoquizMateen ShukriNo ratings yet
- Fibrinolytic Treatment of Complicated Pediatric TDocument2 pagesFibrinolytic Treatment of Complicated Pediatric TDR GURDEEP SINGHNo ratings yet
- 51 Uysal EtalDocument4 pages51 Uysal EtaleditorijmrhsNo ratings yet
- Co-Existence of Pulmonary, Tonsillar and Laryngeal TuberculosisDocument4 pagesCo-Existence of Pulmonary, Tonsillar and Laryngeal TuberculosisSoeHorNo ratings yet
- Sinonasal Eosinophilic Angiocentric FibrosisDocument10 pagesSinonasal Eosinophilic Angiocentric FibrosisPriskila Marlen YoltuwuNo ratings yet
- Jchimp 5 26322Document4 pagesJchimp 5 26322Jongga SiahaanNo ratings yet
- Indian J Radiol Imaging Word 1Document14 pagesIndian J Radiol Imaging Word 1Adie BrianNo ratings yet
- Invasive Aspergillosis in A Patient With End StageDocument8 pagesInvasive Aspergillosis in A Patient With End StageDhurgham QuasimNo ratings yet
- Ofy 038Document5 pagesOfy 038Rosandi AdamNo ratings yet
- Fungal Origin of in Situ Pulmonary Artery Thrombosis: A Case ReportDocument5 pagesFungal Origin of in Situ Pulmonary Artery Thrombosis: A Case ReportIJAR JOURNALNo ratings yet
- X Linked GammaDocument3 pagesX Linked GammaWaseem RajaNo ratings yet
- Letter TO THE Editor: Secondary Organizing Pneumonia After Varicella-Zoster Virus Infection: A Rare AssociationDocument3 pagesLetter TO THE Editor: Secondary Organizing Pneumonia After Varicella-Zoster Virus Infection: A Rare AssociationfatimiahmastaNo ratings yet
- Caso Clinico Clnica Mayo 3Document6 pagesCaso Clinico Clnica Mayo 3Francisco HernandezNo ratings yet
- Chronic Cavitary and Fibrosing Pulmonary and Pleural Aspergillosis: Case Series, Proposed Nomenclature Change, and ReviewDocument16 pagesChronic Cavitary and Fibrosing Pulmonary and Pleural Aspergillosis: Case Series, Proposed Nomenclature Change, and ReviewYassine EssNo ratings yet
- Interstitial Lung Changes in Sjögren's Syndrome: Report of 3 CasesDocument5 pagesInterstitial Lung Changes in Sjögren's Syndrome: Report of 3 CasesRyl WonNo ratings yet
- Simultaneous Bilateral Primary Spontaneous Pneumothorax (2019)Document7 pagesSimultaneous Bilateral Primary Spontaneous Pneumothorax (2019)sandi_prawira_yudhaNo ratings yet
- A Case of Lupus Pneumonitis Mimicking As Infective PneumoniaDocument4 pagesA Case of Lupus Pneumonitis Mimicking As Infective PneumoniaIOSR Journal of PharmacyNo ratings yet
- CytomegaloDocument3 pagesCytomegaloYusi RizkyNo ratings yet
- Infected Pulmonary Infarction Case ReportDocument8 pagesInfected Pulmonary Infarction Case ReportSebastian Felipe Sierra UmañaNo ratings yet
- Rare Cutaneous Tuberculosis FormsDocument6 pagesRare Cutaneous Tuberculosis FormsinggitsiregarNo ratings yet
- A Case of Comorbidity of Complicated Infective Endocarditis and Severe Pneumonia Due To Legionella PneumophilaDocument5 pagesA Case of Comorbidity of Complicated Infective Endocarditis and Severe Pneumonia Due To Legionella PneumophilaSabrina JonesNo ratings yet
- Radiological Findings of Unilateral Tuberculous LuDocument7 pagesRadiological Findings of Unilateral Tuberculous LuSarah watiNo ratings yet
- Neonatal Chronic Bullous Disease and PneumoniaDocument2 pagesNeonatal Chronic Bullous Disease and PneumoniaCharissa Mia D. Salud-GniloNo ratings yet
- Diffuse Large B-Cell Lymphoma Arising From The Lesion ofDocument7 pagesDiffuse Large B-Cell Lymphoma Arising From The Lesion ofFadel AhmadNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Stem Cell-Based Therapy for Lung DiseaseFrom EverandStem Cell-Based Therapy for Lung DiseaseJanette K. BurgessNo ratings yet
- 2017 JAMA Review - Delirium in Older Persons Advances in Diagnosis and Treatment PDFDocument14 pages2017 JAMA Review - Delirium in Older Persons Advances in Diagnosis and Treatment PDFgiseladlrNo ratings yet
- Dog Bite Facts: 4.5 Million Occur Yearly in USDocument5 pagesDog Bite Facts: 4.5 Million Occur Yearly in USDesta KirosNo ratings yet
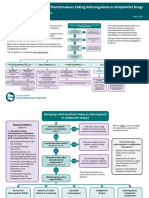
- Sdcep Anticoagulants Quick Reference Guide 2nd EditionDocument5 pagesSdcep Anticoagulants Quick Reference Guide 2nd EditionMeryem LahlouNo ratings yet
- Definition of Infiltration Phlebitis and ExtravasationDocument2 pagesDefinition of Infiltration Phlebitis and ExtravasationJessie YingNo ratings yet
- Clinical PharmacokineticsDocument31 pagesClinical PharmacokineticsArdiyanti Puspitasari100% (1)
- Hafizuddin Azfar (Els 1265)Document46 pagesHafizuddin Azfar (Els 1265)Mohd hafiz AzmiNo ratings yet
- AngiogenesisDocument1 pageAngiogenesisHazim rizkNo ratings yet
- 001 RCA FlipchartDocument40 pages001 RCA FlipchartAbd ZouhierNo ratings yet
- PHS 210 EpidemiologyDocument4 pagesPHS 210 EpidemiologySera GoldNo ratings yet
- Introduction to Pathology of the Skeletal SystemDocument69 pagesIntroduction to Pathology of the Skeletal SystemSoleil SierraNo ratings yet
- Literature Review On Hepatitis B and CDocument10 pagesLiterature Review On Hepatitis B and Cafmzyywqyfolhp100% (1)
- Qu Et Al. 2021Document9 pagesQu Et Al. 2021Kassila SantosNo ratings yet
- David Cesarini Registered Social Worker CV Curriculum VitaeDocument3 pagesDavid Cesarini Registered Social Worker CV Curriculum VitaeDave CesariniNo ratings yet
- Assignment 5.1 OHS Legislation - DiazDocument3 pagesAssignment 5.1 OHS Legislation - DiazADRIAN GABRIEL DIAZNo ratings yet
- Hospital Management System UML and Specification DocumentDocument16 pagesHospital Management System UML and Specification DocumentManish PareekNo ratings yet
- Artesunato MefloquinaDocument11 pagesArtesunato MefloquinaDavid CerrónNo ratings yet
- CroupDocument10 pagesCroupEl Justinson Puspos100% (1)
- Prevention of Waterborne DiseasesDocument2 pagesPrevention of Waterborne DiseasesRixin JamtshoNo ratings yet
- NmghjyjDocument108 pagesNmghjyjindahNo ratings yet
- ARI - Introduction To Medical Varmalogy For Parents of Special ChildrenDocument41 pagesARI - Introduction To Medical Varmalogy For Parents of Special ChildrenArts Research Institute100% (4)
- DysmenorrheaDocument28 pagesDysmenorrheaDr Munira MalikNo ratings yet
- The Coronally Advanced Flap in Combination With Platelet-Rich Fibrin (PRF) and Enamel Matrix Derivative in The Treatment of Gingival Recession: A Comparative StudyDocument15 pagesThe Coronally Advanced Flap in Combination With Platelet-Rich Fibrin (PRF) and Enamel Matrix Derivative in The Treatment of Gingival Recession: A Comparative StudyAnsh Veer ChouhanNo ratings yet
- Job Safety Analysis (JSA) - Painting DateDocument2 pagesJob Safety Analysis (JSA) - Painting DatenabeelNo ratings yet
- 17 TYPES OF GOOD BACTERIA - The List of Most Beneficial Species of Probiotics Lactobacillus and Bifidobacteria - Ecosh LifeDocument30 pages17 TYPES OF GOOD BACTERIA - The List of Most Beneficial Species of Probiotics Lactobacillus and Bifidobacteria - Ecosh LifeCarl MacCordNo ratings yet
- Scenar Testimonials (Updated)Document10 pagesScenar Testimonials (Updated)Tom Askew100% (1)
- Cabizares Handle CaseDocument8 pagesCabizares Handle CaseMae AbabonNo ratings yet
- Asante Teaching Hospital Activity Based CostingDocument3 pagesAsante Teaching Hospital Activity Based CostingMuskanNo ratings yet
- Importance of Health Appraisals for StudentsDocument10 pagesImportance of Health Appraisals for StudentsPantz Revibes PastorNo ratings yet
- AneurysmDocument22 pagesAneurysmRaymond SorianoNo ratings yet
- AOCase Control CohortstudydesignsDocument6 pagesAOCase Control CohortstudydesignsakshayajainaNo ratings yet