You might also like
- The Lidcombe ProgramDocument12 pagesThe Lidcombe ProgramDemosten100% (1)
- Basic Principles of Cancer ChemotherapyDocument2 pagesBasic Principles of Cancer ChemotherapyGerardLum100% (2)
- Consent For Laser Hair RemovalDocument2 pagesConsent For Laser Hair RemovalCassi CrumNo ratings yet
- Introduction To Orthotropics HandbookDocument15 pagesIntroduction To Orthotropics HandbookVio Prico100% (1)
- Jesus Freaks - Dr. Laurence B. BrownDocument3 pagesJesus Freaks - Dr. Laurence B. BrownDany AzizNo ratings yet
- Enteral NutritionDocument18 pagesEnteral NutritionAbdullah YousefNo ratings yet
- 04 Esophageal TumorsDocument36 pages04 Esophageal TumorsDetty NoviantyNo ratings yet
- The Spleen - A Surgical Perspective: by Col. Abrar Hussain ZaidiDocument43 pagesThe Spleen - A Surgical Perspective: by Col. Abrar Hussain Zaidiabrar_zaidiNo ratings yet
- Surgical Diseases of The EsophagusDocument35 pagesSurgical Diseases of The Esophagusmogesie1995No ratings yet
- Thyroidectomy Morbidities:: Preventions & InterventionsDocument52 pagesThyroidectomy Morbidities:: Preventions & InterventionsAlfonso DanacNo ratings yet
- Ca PenisDocument25 pagesCa Penisrajan kumar100% (2)
- Gi Hormones: Dr. Sharon M. PDocument50 pagesGi Hormones: Dr. Sharon M. PAleenaNo ratings yet
- Benign and Malignant Lesion of Lower GIDocument45 pagesBenign and Malignant Lesion of Lower GIAhmad Alzu3beNo ratings yet
- Incisional Hernia RepairDocument6 pagesIncisional Hernia RepairLouis FortunatoNo ratings yet
- Clinical Pracice Guideline For The Treatment of Pediatric Acute Gastroenteritis in The Outpatient SettingDocument8 pagesClinical Pracice Guideline For The Treatment of Pediatric Acute Gastroenteritis in The Outpatient SettingLaura Anghel-MocanuNo ratings yet
- Genital Surgical DiseasesDocument18 pagesGenital Surgical DiseasesanojNo ratings yet
- Bowel PreparationDocument16 pagesBowel PreparationKateAngeliRebosuraNo ratings yet
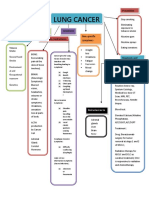
- Concept Map LungDocument1 pageConcept Map LungThea Eya FayeNo ratings yet
- ABSITE CH 10 Nutrition PDFDocument8 pagesABSITE CH 10 Nutrition PDFJames JosephNo ratings yet
- Carcinoma of Lung LectureDocument37 pagesCarcinoma of Lung Lecturesadaf12345678No ratings yet
- Rectum Anus Anatomy 2009 11-3Document38 pagesRectum Anus Anatomy 2009 11-3Ditas ChuNo ratings yet
- TB in Children: Department of Pediatrics College of Medicine Cagayan State UniversityDocument49 pagesTB in Children: Department of Pediatrics College of Medicine Cagayan State UniversityyayayanizaNo ratings yet
- Stomach and Duodenum 10-27Document32 pagesStomach and Duodenum 10-27Ditas ChuNo ratings yet
- Lee Kuan YewDocument12 pagesLee Kuan YewMUSINOV PARVIZNo ratings yet
- Bladder Cancer Structured Reporting Protocol v2 11 FinalDocument88 pagesBladder Cancer Structured Reporting Protocol v2 11 FinaldrelvNo ratings yet
- Lymphadenopathy in ChildrenDocument34 pagesLymphadenopathy in ChildrenAlchemyAdvisory100% (1)
- Graft Vs Host DiseaseDocument44 pagesGraft Vs Host DiseaseHasna Mirda AmazanNo ratings yet
- Ssat Absite Review: HPB: Douglas Cassidy, MD MGH Surgical Education Research and Simulation FellowDocument19 pagesSsat Absite Review: HPB: Douglas Cassidy, MD MGH Surgical Education Research and Simulation FellowmikhailNo ratings yet
- Peptic Ulcer Disease: Dr. Haji Bahadar Pharmd, PHD Assistant Professor Khyber Medical University-PeshawarDocument24 pagesPeptic Ulcer Disease: Dr. Haji Bahadar Pharmd, PHD Assistant Professor Khyber Medical University-Peshawarms khan100% (1)
- EARLY CRC (Peran Bedah Dokter Dalam Diagnosis Dini Karsinoma Kolo-Rectal) Prof - Dr.dr. Ing - Riwanto, SPB-KBDDocument31 pagesEARLY CRC (Peran Bedah Dokter Dalam Diagnosis Dini Karsinoma Kolo-Rectal) Prof - Dr.dr. Ing - Riwanto, SPB-KBDHengky TanNo ratings yet
- Perioperative Chemotherapy (Neoadjuvant or Adjuvant)Document4 pagesPerioperative Chemotherapy (Neoadjuvant or Adjuvant)c.ramNo ratings yet
- Gastrointestinal MalignanciesDocument59 pagesGastrointestinal Malignanciesadamu mohammadNo ratings yet
- Acute Cholecystitis and The Timing of Surgery:: When Is It Time To Heal With Steel?Document48 pagesAcute Cholecystitis and The Timing of Surgery:: When Is It Time To Heal With Steel?Ahmad MullaNo ratings yet
- Opportunistic InfectionsDocument88 pagesOpportunistic InfectionszamadulaNo ratings yet
- Shock (For Surgery)Document50 pagesShock (For Surgery)Emmanuel Rojith VazNo ratings yet
- Chest IntubationDocument42 pagesChest IntubationdrusmanjamilhcmdNo ratings yet
- Poorly Differentiated Thyroid CarcinomaDocument67 pagesPoorly Differentiated Thyroid Carcinomaperie_md100% (1)
- Lecture: Adrenal DisordersDocument78 pagesLecture: Adrenal DisordersOchendo KingxNo ratings yet
- Grafts-Flaps and Tissue TransplantationDocument68 pagesGrafts-Flaps and Tissue Transplantationdaniel situngkir100% (1)
- General Surgery SMALL INTESTINES-Dr MendozaDocument101 pagesGeneral Surgery SMALL INTESTINES-Dr MendozaMedisina101No ratings yet
- Upper Gi BleedDocument20 pagesUpper Gi BleedNaeem Shehzad100% (1)
- β-Lactam Antibiotics: carbapenemsDocument14 pagesβ-Lactam Antibiotics: carbapenemsim. EliasNo ratings yet
- Alvin B. Vibar, M.D.Document49 pagesAlvin B. Vibar, M.D.Ditas ChuNo ratings yet
- Surgical Disease of Spleen Part 2Document52 pagesSurgical Disease of Spleen Part 2Rashed ShatnawiNo ratings yet
- ATA Guideline 2016Document93 pagesATA Guideline 2016Muhammad AndeansahNo ratings yet
- Hepatocellular CarcinomaDocument10 pagesHepatocellular CarcinomaMalueth AnguiNo ratings yet
- Bethesda ScoreDocument7 pagesBethesda ScoreTiberiu BircaNo ratings yet
- Typhoid Ileal Perforation: DR - ArifusmanDocument28 pagesTyphoid Ileal Perforation: DR - ArifusmanMudassar SaeedNo ratings yet
- Paper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionDocument14 pagesPaper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionAimanNo ratings yet
- Anal Canal CarcinomaDocument24 pagesAnal Canal CarcinomaArun guruNo ratings yet
- Abdominal Wall IncisionDocument42 pagesAbdominal Wall IncisionURo KkuNo ratings yet
- Sarcomas of The Head and Neck: Dr. DarwitoDocument60 pagesSarcomas of The Head and Neck: Dr. DarwitolaurasheerNo ratings yet
- Hernia World Conference ProgramDocument112 pagesHernia World Conference ProgramYovan Prakosa100% (1)
- The Pharyngeal Apparatus: - Face, Nasal Cavities, MouthDocument73 pagesThe Pharyngeal Apparatus: - Face, Nasal Cavities, MouthKhasibatul AuliaNo ratings yet
- Abdominal EmergenciesDocument126 pagesAbdominal EmergencieskityamuwesiNo ratings yet
- 06 - Approach To Lymphoma DiagnosisDocument92 pages06 - Approach To Lymphoma DiagnosiscandiddreamsNo ratings yet
- Spindle Cell LesionsDocument8 pagesSpindle Cell LesionsdrmanishsharmaNo ratings yet
- Thymoma: Rawa MuhsinDocument53 pagesThymoma: Rawa MuhsinRawa MuhsinNo ratings yet
- WWW Mcqsurgery ComDocument3 pagesWWW Mcqsurgery ComSajag GuptaNo ratings yet
- Faculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractDocument40 pagesFaculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractGalina LozovanuNo ratings yet
- CA OesophagusDocument47 pagesCA OesophagusAnsif KNo ratings yet
- Bariatric SurgeryDocument26 pagesBariatric SurgeryAmyandNo ratings yet
- Abg Interpretation: Sidra Yousaf, RNDocument37 pagesAbg Interpretation: Sidra Yousaf, RNIhtesham Ul HaqNo ratings yet
- Thyroid CancerDocument39 pagesThyroid CancerFaheem SarwarNo ratings yet
- TUMOURS of ENT PDFDocument7 pagesTUMOURS of ENT PDFShivamNo ratings yet
- Bladder Cancer 1Document31 pagesBladder Cancer 1Anas HamadNo ratings yet
- MPR-MS (Muscle Spasm) - 1299Document1 pageMPR-MS (Muscle Spasm) - 1299DanielleNo ratings yet
- Bereavement: Coping With A DeathDocument28 pagesBereavement: Coping With A DeathTheresa SuleNo ratings yet
- Pulmocare Datasheet For WebsiteDocument1 pagePulmocare Datasheet For WebsiteOanamikaela VaidaNo ratings yet
- The Effectiveness of Physiotherapy After OperativeDocument3 pagesThe Effectiveness of Physiotherapy After OperativeDanny QuezadaNo ratings yet
- Coreg (Carvedilol) 6.25mgDocument3 pagesCoreg (Carvedilol) 6.25mgE100% (2)
- Practical Applications: Crown Lengthening RevisitedDocument7 pagesPractical Applications: Crown Lengthening RevisitedKyoko CPNo ratings yet
- Poster Presentations: 2009 The Authors Journal Compilation 2009 Blackwell Verlag GMBH - Mycoses, 52 (Suppl. 1), 29-123Document95 pagesPoster Presentations: 2009 The Authors Journal Compilation 2009 Blackwell Verlag GMBH - Mycoses, 52 (Suppl. 1), 29-123Flávio VianiNo ratings yet
- Dr. Alon RabinDocument4 pagesDr. Alon RabinDINKER MAHAJANNo ratings yet
- Ainsworth and Bell (1970)Document3 pagesAinsworth and Bell (1970)Chloe100% (2)
- Project On Study The Extent of Self Medication.Document42 pagesProject On Study The Extent of Self Medication.keyurNo ratings yet
- Drug Study HydrocodoneDocument1 pageDrug Study HydrocodoneYlrenne DyNo ratings yet
- Thebestiimulti2022 004Document11 pagesThebestiimulti2022 004Marcin ChłostaNo ratings yet
- Rezitriptan in MigraneDocument19 pagesRezitriptan in MigraneGurdeep SinghNo ratings yet
- Drug StudyDocument2 pagesDrug StudyNURSETOPNOTCHER100% (3)
- MasakoDocument8 pagesMasakoMade UrzuaNo ratings yet
- Price Controls and EntryDocument33 pagesPrice Controls and EntryplatinumadNo ratings yet
- English For NursingDocument32 pagesEnglish For Nursing10Sutra Juita Dewi, Dewa AyuNo ratings yet
- Symptom Management: Chapter Four Denim E. MaghanoyDocument32 pagesSymptom Management: Chapter Four Denim E. MaghanoyDenim Embalzado MaghanoyNo ratings yet
- Hepatic Failure and EncephalopathyDocument4 pagesHepatic Failure and EncephalopathyAnusha VergheseNo ratings yet
- Psoriasis PresentationDocument70 pagesPsoriasis PresentationnunuijoeNo ratings yet
- Torture Treatment Centers - Global Directory 2008Document152 pagesTorture Treatment Centers - Global Directory 2008Coalition for Democracy in IranNo ratings yet
- Drug DoseDocument23 pagesDrug DoserajNo ratings yet
- Masteral PeplauDocument20 pagesMasteral PeplauGinger Enireht HTaibNo ratings yet
- Sr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesDocument41 pagesSr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesNarayanan NMNo ratings yet