You might also like
- Typhoid Ileal Perforation: DR - ArifusmanDocument28 pagesTyphoid Ileal Perforation: DR - ArifusmanMudassar SaeedNo ratings yet
- GRAFT VS HOST AND TRANSPLANT INFECTIONDocument44 pagesGRAFT VS HOST AND TRANSPLANT INFECTIONHasna Mirda AmazanNo ratings yet
- General Surgery SMALL INTESTINES-Dr MendozaDocument101 pagesGeneral Surgery SMALL INTESTINES-Dr MendozaMedisina101No ratings yet
- Surgical Diseases of The EsophagusDocument35 pagesSurgical Diseases of The Esophagusmogesie1995No ratings yet
- Generalanaesthesia Drdhriti 111223120647 Phpapp01Document64 pagesGeneralanaesthesia Drdhriti 111223120647 Phpapp01Ridha Surya NugrahaNo ratings yet
- Chest IntubationDocument42 pagesChest IntubationdrusmanjamilhcmdNo ratings yet
- Opportunistic InfectionsDocument88 pagesOpportunistic InfectionszamadulaNo ratings yet
- Acute Cholecystitis and The Timing of Surgery:: When Is It Time To Heal With Steel?Document48 pagesAcute Cholecystitis and The Timing of Surgery:: When Is It Time To Heal With Steel?Ahmad MullaNo ratings yet
- Lecture: Adrenal DisordersDocument78 pagesLecture: Adrenal DisordersOchendo KingxNo ratings yet
- β-Lactam Antibiotics: carbapenemsDocument14 pagesβ-Lactam Antibiotics: carbapenemsim. EliasNo ratings yet
- The Development of the Pharyngeal Apparatus and FaceDocument73 pagesThe Development of the Pharyngeal Apparatus and FaceKhasibatul AuliaNo ratings yet
- Intestinal Atresia and StenosisDocument7 pagesIntestinal Atresia and StenosisMichael NafarinNo ratings yet
- The Preoperative EvaluationDocument25 pagesThe Preoperative Evaluationnormie littlemonsterNo ratings yet
- Surgical Disease of Spleen Part 2Document52 pagesSurgical Disease of Spleen Part 2Rashed ShatnawiNo ratings yet
- Chylous Fistula of The NeckDocument44 pagesChylous Fistula of The Neckgk_anandaNo ratings yet
- Pyloric Stenosis Guide: Causes, Symptoms, DiagnosisDocument23 pagesPyloric Stenosis Guide: Causes, Symptoms, DiagnosisRama ItachiNo ratings yet
- Interpret ABG ReportsDocument37 pagesInterpret ABG ReportsIhtesham Ul HaqNo ratings yet
- Hernia: Inguinal – Surgical anatomy, presentation, treatment, complicationsDocument43 pagesHernia: Inguinal – Surgical anatomy, presentation, treatment, complicationsFobin VargheseNo ratings yet
- CryptococcosisDocument25 pagesCryptococcosisinvisibleyetinvincibleNo ratings yet
- Fournier's Gangrene EmergencyDocument4 pagesFournier's Gangrene EmergencyLalo ZaraloNo ratings yet
- General AnaestheticsDocument71 pagesGeneral AnaestheticsTamilarasanNo ratings yet
- Disorders of Parathyroid Glands: Hyperparathyroidism and HypoparathyroidismDocument52 pagesDisorders of Parathyroid Glands: Hyperparathyroidism and HypoparathyroidismDr. Akash GuptaNo ratings yet
- Mal RotationDocument13 pagesMal RotationkavyarkrnagarNo ratings yet
- Carcinoma Penis Management GuideDocument63 pagesCarcinoma Penis Management GuideBibek GhimireNo ratings yet
- Reconstruction in Fournier GangreneDocument40 pagesReconstruction in Fournier GangreneAnggie MutmainnahNo ratings yet
- Refkas CondylomaAccuminataDocument18 pagesRefkas CondylomaAccuminatamichelle1945No ratings yet
- Cystic HygromaDocument4 pagesCystic HygromaafrisiammyNo ratings yet
- Hepatitis B: Steve HartDocument36 pagesHepatitis B: Steve HartangelinaNo ratings yet
- Kabwe Central Hospital KCH: Breast Cancer"Document34 pagesKabwe Central Hospital KCH: Breast Cancer"Emmanuel MukukaNo ratings yet
- LiverDocument27 pagesLiverAndi Arwan AgusnawanNo ratings yet
- Excision of Branchial Cleft CystsDocument10 pagesExcision of Branchial Cleft Cystssjs315No ratings yet
- Perioperative ManagementDocument3 pagesPerioperative ManagementRaymond De GulaNo ratings yet
- Benign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraDocument56 pagesBenign Prostate Hyperplasia: Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera UtaraJessica PurbaNo ratings yet
- Skin TumorsDocument56 pagesSkin TumorsAriba Asif100% (1)
- Development of MesentryDocument28 pagesDevelopment of MesentryimmmiNo ratings yet
- Peptic Ulcers GuideDocument46 pagesPeptic Ulcers GuideEmmanuel MukukaNo ratings yet
- Thyroid Disorders: Types, Symptoms, and TreatmentsDocument41 pagesThyroid Disorders: Types, Symptoms, and Treatmentssheila_kohNo ratings yet
- Suprarenal (Adrenal) Gland: Dr. R. SanthakumarDocument33 pagesSuprarenal (Adrenal) Gland: Dr. R. SanthakumardrsubanNo ratings yet
- Management of Acute and Chronic Urinary RetentionDocument52 pagesManagement of Acute and Chronic Urinary RetentionSri HariNo ratings yet
- Anaesthesia in Liver Disease PatientDocument49 pagesAnaesthesia in Liver Disease PatientVG FernandezNo ratings yet
- Differential Diagnosis Pain Right HypochondriumDocument35 pagesDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- Patient Positioning During AnaesthesiaDocument6 pagesPatient Positioning During AnaesthesiaDarman ZulfikarNo ratings yet
- Tracheostomy Procedure GuideDocument10 pagesTracheostomy Procedure GuideAinur AbdrakhmanovaNo ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument28 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNo ratings yet
- Drug-Induced QT Interval ProlongationDocument13 pagesDrug-Induced QT Interval ProlongationgeoaislaNo ratings yet
- Sarcomas of The Head and Neck: Dr. DarwitoDocument60 pagesSarcomas of The Head and Neck: Dr. DarwitolaurasheerNo ratings yet
- CURRENT STATUS of HAL-RAR (Haemorrhoids Casee and Treatment in Indonesia) Prof - Dr.dr. Ing - Riwanto, SPB-KBDDocument43 pagesCURRENT STATUS of HAL-RAR (Haemorrhoids Casee and Treatment in Indonesia) Prof - Dr.dr. Ing - Riwanto, SPB-KBDHengky TanNo ratings yet
- Histology Lower GIT Microscopic Features Small Large IntestineDocument27 pagesHistology Lower GIT Microscopic Features Small Large IntestineArwa100% (2)
- Carcinoma of The Breast - Bailey & LoveDocument5 pagesCarcinoma of The Breast - Bailey & LoveKeyshia Yazid100% (1)
- Local AnaestheticsDocument26 pagesLocal Anaestheticsv_vijayakanth7656No ratings yet
- Abdominal Wall Extraskeletal Ewing Sarcoma - Case ReportDocument3 pagesAbdominal Wall Extraskeletal Ewing Sarcoma - Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- Anatomy of the OesophagusDocument28 pagesAnatomy of the OesophagusAbdur RaqibNo ratings yet
- 13Lec-Approach To Neonates With Suspected Congenital InfectionsDocument56 pages13Lec-Approach To Neonates With Suspected Congenital InfectionsMinerva Stanciu100% (1)
- HerniaDocument16 pagesHerniaVetrivel TamizhNo ratings yet
- BarotraumaDocument15 pagesBarotraumaEfa YusufNo ratings yet
- Seminar-Surgical Infection and Antibiotic PolicyDocument92 pagesSeminar-Surgical Infection and Antibiotic Policyaslan100% (1)
- Acute Pyelonephritis Treatment GuidelinesDocument4 pagesAcute Pyelonephritis Treatment GuidelinesPeter InocandoNo ratings yet
- Back To Basics Fundamentals of Wound Care and Dressing Selection Spring WorkshopDocument43 pagesBack To Basics Fundamentals of Wound Care and Dressing Selection Spring WorkshopBima Achmad100% (1)
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- Bss1 - Indonesia - Share2018Document43 pagesBss1 - Indonesia - Share2018Michael RaktionNo ratings yet
- Contoh Laporan Skrining SRQ-29Document6 pagesContoh Laporan Skrining SRQ-29daniel situngkirNo ratings yet
- 1Chp6 Ocular Surface DiseasesDocument31 pages1Chp6 Ocular Surface DiseasesKartika RezkyNo ratings yet
- 6 - Lipid U - Guidelines - JonesDocument48 pages6 - Lipid U - Guidelines - Jonesdaniel situngkirNo ratings yet
- Dry Eye Syndrome PPPDocument44 pagesDry Eye Syndrome PPPHendra GunawanNo ratings yet
- VandAToolkit Mod2 Powerpoint 508 PDFDocument40 pagesVandAToolkit Mod2 Powerpoint 508 PDFdaniel situngkirNo ratings yet
- RdsDocument6 pagesRdsOlivia Valentine LekiNo ratings yet
- Chapter 19 Respiratory Distress SyndrDocument9 pagesChapter 19 Respiratory Distress SyndrPatrick Larbi Awuku100% (1)
- European Consensus Guidelines On The%2Document16 pagesEuropean Consensus Guidelines On The%2Marce ColmeneroNo ratings yet
- 2015 AHA Guidelines Highlights EnglishDocument36 pages2015 AHA Guidelines Highlights EnglishshiloinNo ratings yet
- 2015 AHA Guidelines Highlights EnglishDocument36 pages2015 AHA Guidelines Highlights EnglishshiloinNo ratings yet
- AF AWARE Workshop: Note To Members: Should You Choose To Use These Slides, Please Acknowledge The Original AuthorsDocument77 pagesAF AWARE Workshop: Note To Members: Should You Choose To Use These Slides, Please Acknowledge The Original Authorsdaniel situngkirNo ratings yet
- Skin Grafts: BY DR - Surapol ChagkornbureeDocument30 pagesSkin Grafts: BY DR - Surapol Chagkornbureedaniel situngkirNo ratings yet
- Guidelines SLCM BWDocument60 pagesGuidelines SLCM BWpnaarayanNo ratings yet
- Thermo Safety Cabinets MSC-Advantage - User ManualDocument53 pagesThermo Safety Cabinets MSC-Advantage - User ManualAhmed SalamaNo ratings yet
- What Is Managerial Economics? Explain Its Nature, Scope and ItsDocument9 pagesWhat Is Managerial Economics? Explain Its Nature, Scope and Itsn13shukla85% (20)
- Mercer Role and Job Analysis InfoDocument3 pagesMercer Role and Job Analysis InfojehaniaNo ratings yet
- 1 Catalyst FundamentalsDocument17 pages1 Catalyst FundamentalsSam AnuNo ratings yet
- LAWO PI - MADI - SRC - enDocument2 pagesLAWO PI - MADI - SRC - enfjavierpoloNo ratings yet
- Acrogym: by Ahana AnandDocument9 pagesAcrogym: by Ahana AnandAhana AnandNo ratings yet
- Sony STR Da80esDocument66 pagesSony STR Da80estelstarservicesNo ratings yet
- VLSI Implementation of Floating Point AdderDocument46 pagesVLSI Implementation of Floating Point AdderParamesh Waran100% (1)
- Man 400eDocument324 pagesMan 400eLopez Tonny100% (1)
- User Manual: Rider 320Document46 pagesUser Manual: Rider 320SarahNo ratings yet
- Trisomy 21 An Understanding of The DiseaseDocument28 pagesTrisomy 21 An Understanding of The DiseaseHannahjane YbanezNo ratings yet
- PTR01 21050 90inst PDFDocument40 pagesPTR01 21050 90inst PDFЯн ПавловецNo ratings yet
- Compiler Design and Linux System AdministrationDocument47 pagesCompiler Design and Linux System AdministrationGouri ShankerNo ratings yet
- 1866 Lee Animal Magnetism and Magnet Lucid SomnambulismDocument354 pages1866 Lee Animal Magnetism and Magnet Lucid SomnambulismtvosNo ratings yet
- Engineering Design For A Circular Economy - A List of Design GuidelinesDocument1 pageEngineering Design For A Circular Economy - A List of Design Guidelinesmy oneNo ratings yet
- Price Action - Japanese Candlestick Patterns SheetDocument4 pagesPrice Action - Japanese Candlestick Patterns SheetVicaas VSNo ratings yet
- OYO Case Study SolutionDocument4 pagesOYO Case Study SolutionVIKASH GARGNo ratings yet
- Semiconductor Optical AmplifierDocument40 pagesSemiconductor Optical AmplifierVikas ThakurNo ratings yet
- Lab Practice # 01 An Introduction To MatlabDocument10 pagesLab Practice # 01 An Introduction To MatlabGhulam Abbas LashariNo ratings yet
- Toyota Genuine ATF WSDocument14 pagesToyota Genuine ATF WSKirillNo ratings yet
- But Virgil Was Not There": The Lasting Impact of Dante's Homosocial HellDocument7 pagesBut Virgil Was Not There": The Lasting Impact of Dante's Homosocial HellЮлия ЧебанNo ratings yet
- 2006fileaveo MTDocument63 pages2006fileaveo MTeurospeed2100% (1)
- What ATF - CVTF To Use For ToyotaDocument7 pagesWhat ATF - CVTF To Use For ToyotaSydneyKasongoNo ratings yet
- Sop For FatDocument6 pagesSop For Fatahmed ismailNo ratings yet
- 5.test Report - RFU-C-7Ghz IP10 Extract VersionDocument42 pages5.test Report - RFU-C-7Ghz IP10 Extract Versionminhdung.pham4713No ratings yet
- PDA Technical Documents on Sterilization ProcessesDocument3 pagesPDA Technical Documents on Sterilization ProcessesManas MishraNo ratings yet
- Course Code Part Sem Paper Code Paper NameDocument3 pagesCourse Code Part Sem Paper Code Paper Nameshiv mishraNo ratings yet
- String inverter comparisonDocument4 pagesString inverter comparisonRakesh HateyNo ratings yet
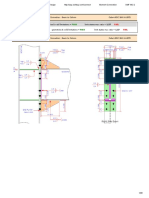
- Result Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDDocument29 pagesResult Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDYash Suthar100% (2)