You might also like
- Statistical Analysis PlanDocument92 pagesStatistical Analysis PlanhimeshagrawalNo ratings yet
- London Medicines Evaluation Network Reviews Pharmacokinetic Profiles of Extended-Release MethylphenidateDocument9 pagesLondon Medicines Evaluation Network Reviews Pharmacokinetic Profiles of Extended-Release Methylphenidateassajadda lizikriNo ratings yet
- Catalyst RX Formulary IntroductionDocument4 pagesCatalyst RX Formulary IntroductionRahul MishraNo ratings yet
- AL y Signos VitalesDocument7 pagesAL y Signos VitalesPedro Jose Rios GNo ratings yet
- Guía de Dosis de AntipsicóticosDocument8 pagesGuía de Dosis de AntipsicóticoskarlunchoNo ratings yet
- Medoral 21 E579Document8 pagesMedoral 21 E579AngiPaolaPuiconRuizNo ratings yet
- Anesth Analg-2012-Corcoran-640-51 PDFDocument12 pagesAnesth Analg-2012-Corcoran-640-51 PDFBijay KCNo ratings yet
- Open Label Clinical Study To Evaluate The Safety and Tolerability of TreprostinilDocument14 pagesOpen Label Clinical Study To Evaluate The Safety and Tolerability of TreprostinilMaria Jose Contreras SilvaNo ratings yet
- DTH 14650Document19 pagesDTH 14650Evelyn LimNo ratings yet
- Premedication With Oral Tramadol Reduces Severity of Postoperative Shivering After General AnesthesiaDocument6 pagesPremedication With Oral Tramadol Reduces Severity of Postoperative Shivering After General AnesthesiaFajar NarakusumaNo ratings yet
- JeradDocument10 pagesJeradzaimmuhtarNo ratings yet
- FentanylDocument12 pagesFentanylUtomo FemtomNo ratings yet
- 0300060513485864Document11 pages0300060513485864Aashish KalikaNo ratings yet
- Medication Use During End-Of-Life Care in A Palliative Care CentreDocument9 pagesMedication Use During End-Of-Life Care in A Palliative Care CentreCaio CandidoNo ratings yet
- Medication Assisted Treatment of Opioid Use.2Document13 pagesMedication Assisted Treatment of Opioid Use.2tatanmenaNo ratings yet
- The Effectsof Diaphragmatic Breathingand Omeprazoleon Respiratory Indicesand Diaphragmatic Excursionin Patientswith Gastroesophageal Reflux DiseaseDocument6 pagesThe Effectsof Diaphragmatic Breathingand Omeprazoleon Respiratory Indicesand Diaphragmatic Excursionin Patientswith Gastroesophageal Reflux DiseaseSHAFANA PUTRI -No ratings yet
- Dexketoprofen/tramadol: Randomised Double-Blind Trial and Confirmation of Empirical Theory of Combination Analgesics in Acute PainDocument13 pagesDexketoprofen/tramadol: Randomised Double-Blind Trial and Confirmation of Empirical Theory of Combination Analgesics in Acute PainskripsianiNo ratings yet
- Research: Corticosteroids For Pain Relief in Sore Throat: Systematic Review and Meta-AnalysisDocument7 pagesResearch: Corticosteroids For Pain Relief in Sore Throat: Systematic Review and Meta-AnalysiswindaintanpNo ratings yet
- Respiratory ResearchDocument32 pagesRespiratory ResearchNuno DuarteNo ratings yet
- Lack of Efficacy of Long-Term, Low-Dose Azithromycin in Chronic Rhinosinusitis: A Randomized Controlled TrialDocument12 pagesLack of Efficacy of Long-Term, Low-Dose Azithromycin in Chronic Rhinosinusitis: A Randomized Controlled Trialpaijo09No ratings yet
- Disertasi BiofarmasiDocument167 pagesDisertasi BiofarmasiJerry Skate RasBebasNo ratings yet
- Theobromine Inhibits CoughDocument16 pagesTheobromine Inhibits CoughRaffaello MobiliaNo ratings yet
- Adalimumab added to methotrexate increases remission in early rheumatoid arthritisDocument10 pagesAdalimumab added to methotrexate increases remission in early rheumatoid arthritisElenaChiriacovaNo ratings yet
- 2019 A&a Dez MetadonaDocument3 pages2019 A&a Dez MetadonajaquelinemiyakeNo ratings yet
- A comparison of midazolam and diazepam for dental sedationDocument5 pagesA comparison of midazolam and diazepam for dental sedationGu GuuNo ratings yet
- Ncologist: R I FDADocument7 pagesNcologist: R I FDAapi-26302710No ratings yet
- Ijohns 2015031219070250Document9 pagesIjohns 2015031219070250listyaNo ratings yet
- AminoglicozideDocument7 pagesAminoglicozideDiana Mihaela BadescuNo ratings yet
- Cerminara Et Al 2017 A Single Center Retrospective Analysis of A Protocol For High Dose Methotrexate and LeucovorinDocument9 pagesCerminara Et Al 2017 A Single Center Retrospective Analysis of A Protocol For High Dose Methotrexate and Leucovorinanton.neonatusNo ratings yet
- PIIS2213260017304745Document10 pagesPIIS2213260017304745Juan Pablo CasanovaNo ratings yet
- Journal - Medication Dry Mounth 2018 - Tan EdwinDocument9 pagesJournal - Medication Dry Mounth 2018 - Tan EdwinranisaNo ratings yet
- Drug Delivery Systems - An Update ReviewDocument10 pagesDrug Delivery Systems - An Update ReviewenzomontresolNo ratings yet
- Comparative in Vitro Dissolution and in Vivo Bioequivalence of Two Diclofenac Enteric Coated FormulationsDocument5 pagesComparative in Vitro Dissolution and in Vivo Bioequivalence of Two Diclofenac Enteric Coated FormulationsgeoaislaNo ratings yet
- Ropvacaina VS Lidocaina Premdicacion IotDocument6 pagesRopvacaina VS Lidocaina Premdicacion IotFaith Lu PenalozaNo ratings yet
- Background: Pharmacotherapy For Hypertension in Women of Different RacesDocument6 pagesBackground: Pharmacotherapy For Hypertension in Women of Different RacesRisma S PNo ratings yet
- Menyhei 1994Document4 pagesMenyhei 1994Anett Pappné LeppNo ratings yet
- Hope 4 Lancet 2019Document12 pagesHope 4 Lancet 2019Marco Cordova RosellNo ratings yet
- Timing is important in medication administration; a timely review of chronotherapy researchDocument15 pagesTiming is important in medication administration; a timely review of chronotherapy researchCarlos RomeroNo ratings yet
- The Role of Dexmedetomidine (Precedex) in The Sedation of Critically Ill PatientsDocument4 pagesThe Role of Dexmedetomidine (Precedex) in The Sedation of Critically Ill Patientspshz05No ratings yet
- 223 2012 Article 9639Document10 pages223 2012 Article 9639Daniela CerianiNo ratings yet
- Introduction: Intravenous Ibuprofen May Offer Advantages Over Ketorolac For Postoperative Pain ControlDocument6 pagesIntroduction: Intravenous Ibuprofen May Offer Advantages Over Ketorolac For Postoperative Pain ControlnadaNo ratings yet
- Methamphetamine and Amphetamine Pharmacokinetics in Oral Fluid and Plasma After Controlled Oral Methamphetamine Administration To Human VolunteersDocument12 pagesMethamphetamine and Amphetamine Pharmacokinetics in Oral Fluid and Plasma After Controlled Oral Methamphetamine Administration To Human VolunteersemmypuspitasariNo ratings yet
- Medoral 20 E459Document5 pagesMedoral 20 E459Tania RodriguezNo ratings yet
- Receptor Antagonist, Asthma, Seratrodast, Montelukast, Peak Expiratory Flow (PEF), Eosinophil Cationic Protein (ECP), AlbuminDocument10 pagesReceptor Antagonist, Asthma, Seratrodast, Montelukast, Peak Expiratory Flow (PEF), Eosinophil Cationic Protein (ECP), AlbuminZuventusHealthcareNo ratings yet
- MeduriDocument4 pagesMeduriSilvia Leticia BrunoNo ratings yet
- AnestesiDocument17 pagesAnestesibodroNo ratings yet
- Systematic Review and Network Meta-Analysis of Stroke Prevention Treatments in Patients With Atrial FibrillationDocument15 pagesSystematic Review and Network Meta-Analysis of Stroke Prevention Treatments in Patients With Atrial FibrillationAlicePastranaNo ratings yet
- A Double-Blind Randomized Controlled Trial of Normal Saline, Lactated Ringer's, and Hypertonic Saline Nasal Irrigation Solution After Endoscopic Sinus SurgeryDocument7 pagesA Double-Blind Randomized Controlled Trial of Normal Saline, Lactated Ringer's, and Hypertonic Saline Nasal Irrigation Solution After Endoscopic Sinus SurgeryYasdika ImamNo ratings yet
- Evaluation of The Buccal Vestibule-Palatal Diffusion of 4% Articaine Hydrochloride in Impacted Maxillary Third Molar ExtractionsDocument4 pagesEvaluation of The Buccal Vestibule-Palatal Diffusion of 4% Articaine Hydrochloride in Impacted Maxillary Third Molar ExtractionsDRPRIYA007No ratings yet
- Three Anxiety Protocols Compared for Tooth ExtractionDocument8 pagesThree Anxiety Protocols Compared for Tooth ExtractionDiego LemurNo ratings yet
- Pharmacokinetics of Oral and Intravenous Paracetamol (Acetaminophen) When Co-Administered With Intravenous Morphine in Healthy Adult SubjectsDocument10 pagesPharmacokinetics of Oral and Intravenous Paracetamol (Acetaminophen) When Co-Administered With Intravenous Morphine in Healthy Adult SubjectsRara MaharrumNo ratings yet
- The Effect of Delmopinol Mouthwash On Aphthous StomatitisDocument19 pagesThe Effect of Delmopinol Mouthwash On Aphthous StomatitisAthenaeum Scientific PublishersNo ratings yet
- A Career in The Pharmaceutical SciencesDocument19 pagesA Career in The Pharmaceutical SciencesDrSandeep NarulaNo ratings yet
- Mephedrone Pharmacokinetics After Intravenous and Oral Administration in Rats: Relation To PharmacodynamicsDocument23 pagesMephedrone Pharmacokinetics After Intravenous and Oral Administration in Rats: Relation To PharmacodynamicsReal GuruNo ratings yet
- Remifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized StudyDocument7 pagesRemifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized Studyade_liaNo ratings yet
- Jced 7 E84Document5 pagesJced 7 E84Karina HernandezNo ratings yet
- M34 16Document2 pagesM34 16Ana Tomas PetrovicNo ratings yet
- Ismail 2013Document6 pagesIsmail 2013Nawang WulanNo ratings yet
- Antiepileptic Drugs-Best Practice Guidelines ForDocument38 pagesAntiepileptic Drugs-Best Practice Guidelines ForAbraham Escobedo MoratillaNo ratings yet
- A Model Informed Method For The Purpose of Precision Dosing of Isoniazid in Pulmonary TuberculosisDocument11 pagesA Model Informed Method For The Purpose of Precision Dosing of Isoniazid in Pulmonary TuberculosisNitish TankNo ratings yet
- Parakh 2017Document5 pagesParakh 2017Muhammad Ali Syahrun MubarokNo ratings yet
- Trenaxamic AcidDocument9 pagesTrenaxamic AciddesyhavizhahNo ratings yet
- Pro DrugsDocument46 pagesPro DrugsAditya KotamrajuNo ratings yet
- Research Triangle Regions Life Sciences Directory 2012Document50 pagesResearch Triangle Regions Life Sciences Directory 2012hitexNo ratings yet
- Indian Pharmacopoeia Download PDFDocument3 pagesIndian Pharmacopoeia Download PDFManuel Alberto Castillo Aguirre25% (4)
- Drug effects and clinical trials overviewDocument1 pageDrug effects and clinical trials overviewKlare TyNo ratings yet
- Farmakokinetika 1Document19 pagesFarmakokinetika 1Sari Ranial ZhaptaNo ratings yet
- Pyy 071Document16 pagesPyy 071Stella SulartoNo ratings yet
- of M.pharmDocument13 pagesof M.pharmVivek Patel ViksNo ratings yet
- The Production of MedicinesDocument9 pagesThe Production of MedicinesAngelNo ratings yet
- Course Curriculum EwuDocument4 pagesCourse Curriculum EwudearshuvroNo ratings yet
- Butilbromuro de Hioscina Una Revisión de Su Uso en El Tratamiento de Cólicos y Dolor AbdominalDocument6 pagesButilbromuro de Hioscina Una Revisión de Su Uso en El Tratamiento de Cólicos y Dolor AbdominalalexqaNo ratings yet
- Storage and Transportation of Investigational Drug ProductsDocument4 pagesStorage and Transportation of Investigational Drug ProductsDilawar BakhtNo ratings yet
- Drugs and The BodyDocument5 pagesDrugs and The BodyValones BeaNo ratings yet
- FDA Draft Guidance on Bioequivalence Studies for Dienogest; Estradiol ValerateDocument2 pagesFDA Draft Guidance on Bioequivalence Studies for Dienogest; Estradiol ValerateAna BelgaNo ratings yet
- Pharmacokinetic ParametersDocument29 pagesPharmacokinetic Parametersfaisalnadeem100% (1)
- Week4 PTC Formulary DispensingDocument7 pagesWeek4 PTC Formulary DispensingChunnie JakosalemNo ratings yet
- Rebamipide, A Gastro-Protective and Anti-Inflammatory Drug, Promotes Gastric Ulcer Healing Following Eradication TherapyDocument4 pagesRebamipide, A Gastro-Protective and Anti-Inflammatory Drug, Promotes Gastric Ulcer Healing Following Eradication TherapySilvester HenryNo ratings yet
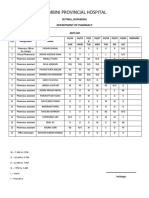
- Lumbini Provincial Hospital: Department of PharmacyDocument2 pagesLumbini Provincial Hospital: Department of PharmacyImdadHussainOPositiveNo ratings yet
- p1 PDFDocument79 pagesp1 PDFJames PerianayagamNo ratings yet
- Nearest Pharmacy Delivery ServiceDocument5 pagesNearest Pharmacy Delivery ServiceJayanath SamarasingheNo ratings yet
- UntitledDocument12 pagesUntitledjhony192No ratings yet
- Cpdprogram Pharmacy 82318Document81 pagesCpdprogram Pharmacy 82318PRC BoardNo ratings yet
- TDM UtsDocument285 pagesTDM Utsnabila auliaNo ratings yet
- PRELIMSDocument21 pagesPRELIMSPrincess NicoleNo ratings yet
- Rancangan Dan Pengembangan FormulaDocument60 pagesRancangan Dan Pengembangan FormulaI M BrotoNo ratings yet
- Pharmaceutical absorption and bioavailabilityDocument18 pagesPharmaceutical absorption and bioavailabilityFredNo ratings yet
- PHARMECUETICALDocument3 pagesPHARMECUETICALgaming loverNo ratings yet
- ADMINISTRATIVE ORDER No. 144 S. 2004Document2 pagesADMINISTRATIVE ORDER No. 144 S. 2004Mae GandaNo ratings yet