0% found this document useful (0 votes)
17 views3 pagesJob Embedded Learning
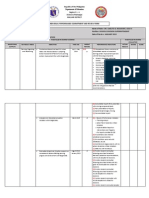
The document outlines an evaluation form for training participants, focusing on their action plans and job-embedded learning. It includes a rating system for assessing the effectiveness of the action plan and the competencies demonstrated by participants. Additionally, there is a section for documenting critical incidents that showcase competencies not captured in the questionnaire.
Uploaded by
ritchel mag-aboCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
17 views3 pagesJob Embedded Learning
The document outlines an evaluation form for training participants, focusing on their action plans and job-embedded learning. It includes a rating system for assessing the effectiveness of the action plan and the competencies demonstrated by participants. Additionally, there is a section for documenting critical incidents that showcase competencies not captured in the questionnaire.
Uploaded by
ritchel mag-aboCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd