You might also like
- Functional Limitations and Developmental DelaysDocument64 pagesFunctional Limitations and Developmental DelaysTinaHoNo ratings yet
- Fetal Alcohol Spectrum Disorders: The BasicsDocument42 pagesFetal Alcohol Spectrum Disorders: The BasicsAshok Kumar KrishnamoorthyNo ratings yet
- The Role of The Social Worker in Preventing, Identifying and Treating FASDDocument49 pagesThe Role of The Social Worker in Preventing, Identifying and Treating FASDfasdunited100% (2)
- Fetal Alcohol SyndromeDocument9 pagesFetal Alcohol Syndromeapi-302579319No ratings yet
- Attention Deficit Hyperactivity Disorder in Children & AdolescentsDocument68 pagesAttention Deficit Hyperactivity Disorder in Children & AdolescentsSiva KumarrNo ratings yet
- 2) Growth & DevelopmentDocument61 pages2) Growth & DevelopmentNu JoeNo ratings yet
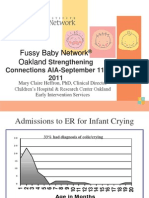
- Fussy Baby Presentation - AustinDocument55 pagesFussy Baby Presentation - AustinSutarmi SutarmiNo ratings yet
- F.2 Separation Anxiety PPT 2017Document33 pagesF.2 Separation Anxiety PPT 2017Ptrc Lbr LpNo ratings yet
- Asd and Adhd (Week 16)Document57 pagesAsd and Adhd (Week 16)Krisha Mabel TabijeNo ratings yet
- Adepoju - Failure To ThriveDocument37 pagesAdepoju - Failure To ThriveAdepoju Victor AbiolaNo ratings yet
- Fetal Alcohol Spectrum Disorders - What Is ItDocument5 pagesFetal Alcohol Spectrum Disorders - What Is ItgemaNo ratings yet
- Austism Spectrum DisorderDocument21 pagesAustism Spectrum DisorderFrancez Anne GuanzonNo ratings yet
- F.5 Selective Mutism Powerpoint 2016Document32 pagesF.5 Selective Mutism Powerpoint 2016Ptrc Lbr LpNo ratings yet
- Child PsychologyDocument16 pagesChild PsychologyDimple BorahNo ratings yet
- Intellectual Disability/ Mental Retardation: Level IV Tutorial 2015/2016 DR J. KamauDocument21 pagesIntellectual Disability/ Mental Retardation: Level IV Tutorial 2015/2016 DR J. KamauRahul Kumar DiwakarNo ratings yet
- Child DisordersDocument111 pagesChild Disorderspriyanka rajNo ratings yet
- FASD Brochure For Teachers: Aint MisbehavingDocument2 pagesFASD Brochure For Teachers: Aint Misbehavingfasdunited100% (2)
- Autism: By: Chloe' HanesDocument10 pagesAutism: By: Chloe' HanesKhairil AzwarNo ratings yet
- Issues and Challenges On DevelopmentDocument24 pagesIssues and Challenges On DevelopmentMaria MariaNo ratings yet
- Autism Spectrum Disorder With Videos 2022 - FAYDocument26 pagesAutism Spectrum Disorder With Videos 2022 - FAYNikky SilvestreNo ratings yet
- Intellectual Disability/Mental Retardation: Presented By: Miahlee Madrid & Rose Ann PadillaDocument32 pagesIntellectual Disability/Mental Retardation: Presented By: Miahlee Madrid & Rose Ann PadillazsanikaNo ratings yet
- Approach To Developmental DelayDocument35 pagesApproach To Developmental DelayAadil AminNo ratings yet
- Fetal Alcohol Syndrome: Causes, Symptoms and PreventionDocument12 pagesFetal Alcohol Syndrome: Causes, Symptoms and Preventionezra.itaasNo ratings yet
- Child and Adolescent DisordersDocument49 pagesChild and Adolescent DisordersKirsten Padilla ChuaNo ratings yet
- Attention Deficit and Learning DisablilesDocument36 pagesAttention Deficit and Learning DisablilesNatearia ThrowerNo ratings yet
- Learning Disabilities ExplainedDocument20 pagesLearning Disabilities ExplainedSùjâl PätídàrNo ratings yet
- Fetal Alcohol SyndromeDocument11 pagesFetal Alcohol SyndromeMerlin AllenNo ratings yet
- Unit VII Assessment of The Pediatric ClientDocument36 pagesUnit VII Assessment of The Pediatric ClientSyed Maaz100% (1)
- Children With Special NeedsDocument29 pagesChildren With Special NeedsOmyNo ratings yet
- Affect EducationDocument12 pagesAffect EducationLeany AurelioNo ratings yet
- Disruptive Behaviour Disorders: Donna Dowling Child & Adolescent Psychiatrist Townsville CAYASDocument76 pagesDisruptive Behaviour Disorders: Donna Dowling Child & Adolescent Psychiatrist Townsville CAYASVukashin.meNo ratings yet
- Peds History (C FW06)Document35 pagesPeds History (C FW06)Prasad RauNo ratings yet
- Common Child Psychiatric DisordersDocument30 pagesCommon Child Psychiatric DisordersabrihamNo ratings yet
- Fetal Alcohol SyndromeDocument30 pagesFetal Alcohol SyndromeTwilight GamingNo ratings yet
- Understanding Intellectual DisabilityDocument32 pagesUnderstanding Intellectual DisabilityVince Baring DelantarNo ratings yet
- Student Unit 2 Topic 2.6 Jan 2018Document14 pagesStudent Unit 2 Topic 2.6 Jan 2018Krista KloseNo ratings yet
- Failure To Thrive (FTT)Document23 pagesFailure To Thrive (FTT)Endrow Francisco100% (1)
- محاضرة 9 Psychology of Handicaped دبلوم ع وظيفيDocument27 pagesمحاضرة 9 Psychology of Handicaped دبلوم ع وظيفيNour ElsabahNo ratings yet
- Children With Disabilities: Experiences, ChallengesDocument28 pagesChildren With Disabilities: Experiences, ChallengesFilja JohnNo ratings yet
- Matt WoolgarDocument36 pagesMatt WoolgarafteradoptionNo ratings yet
- Fetal Alcohol Syndrome - Scenario Power PointDocument13 pagesFetal Alcohol Syndrome - Scenario Power PointShaheen324No ratings yet
- Attention Deficit Hyperactivity Disorder (ADHD)Document47 pagesAttention Deficit Hyperactivity Disorder (ADHD)HarisSafiNo ratings yet
- Early Identification and Screening: Definition of Developmental DelayDocument7 pagesEarly Identification and Screening: Definition of Developmental Delayadheena simonNo ratings yet
- ResourceManual MateoDocument3 pagesResourceManual MateoKimLawrence MulatoNo ratings yet
- Development in Down SyndromeDocument30 pagesDevelopment in Down SyndromeRoilan MarlangNo ratings yet
- Child Clinical Interview Form OnlineDocument24 pagesChild Clinical Interview Form OnlineMonica Bolocan100% (3)
- Global Developmental DelayedDocument20 pagesGlobal Developmental DelayedabrararbhiwaNo ratings yet
- Webinar Slides: Eileen Elias, M. Ed. and Douglas Waite, M.D.Document28 pagesWebinar Slides: Eileen Elias, M. Ed. and Douglas Waite, M.D.fasdunited100% (1)
- Common Childhood Mental Disorders Explained/TITLEDocument42 pagesCommon Childhood Mental Disorders Explained/TITLEMsm BeihoNo ratings yet
- Behavioral & Developmental VariationsDocument57 pagesBehavioral & Developmental Variationsapi-19641337No ratings yet
- Case History Form-1Document27 pagesCase History Form-1....No ratings yet
- Mental RetardationDocument14 pagesMental RetardationSumam NeveenNo ratings yet
- Anamnesia EnglishDocument33 pagesAnamnesia EnglishMalikNo ratings yet
- Child Abuse: Risks, Signs, and ReportingDocument16 pagesChild Abuse: Risks, Signs, and Reportingakkineni ruchithaNo ratings yet
- Causes of Exceptionality: Intellectual Disability, Autism, Hearing LossDocument4 pagesCauses of Exceptionality: Intellectual Disability, Autism, Hearing LossMalik FauzNo ratings yet
- Microcephaly PresentationDocument22 pagesMicrocephaly PresentationBinita ShresthaNo ratings yet
- 1 07a-NeurodevDocument75 pages1 07a-NeurodevNirav CHOVATIYANo ratings yet
- Genetic CounselingDocument24 pagesGenetic Counselinglaksshanya50% (2)
- Physical & Cognitive Development of Tweens: Psychology 307, Development Guest Lecture 3/24/09 Eswen FavaDocument10 pagesPhysical & Cognitive Development of Tweens: Psychology 307, Development Guest Lecture 3/24/09 Eswen FavaPriska ValiniaNo ratings yet
- 3-Bioelectrical Stimulation For People With Patterns Consistent With Certain Chronic InfectionsDocument8 pages3-Bioelectrical Stimulation For People With Patterns Consistent With Certain Chronic InfectionsSaad MotawéaNo ratings yet
- Outbreak Investigation Monday's ExerciseDocument5 pagesOutbreak Investigation Monday's ExerciseSaad MotawéaNo ratings yet
- Wong F Food OverviewDocument25 pagesWong F Food OverviewSaad MotawéaNo ratings yet
- Biological WeaponsDocument29 pagesBiological WeaponsSaad Motawéa100% (1)
- Session 1 - BT Epi Response Training - Outbreak InvestigationDocument41 pagesSession 1 - BT Epi Response Training - Outbreak InvestigationSaad MotawéaNo ratings yet
- 2-Electrotherapy For Blood ElectrificationDocument12 pages2-Electrotherapy For Blood ElectrificationSaad MotawéaNo ratings yet
- Giardia BenchaidDocument2 pagesGiardia BenchaidSaad MotawéaNo ratings yet
- 3-Bioelectrical Stimulation For People With Patterns Consistent With Certain Chronic InfectionsDocument8 pages3-Bioelectrical Stimulation For People With Patterns Consistent With Certain Chronic InfectionsSaad MotawéaNo ratings yet
- Investigating OutbreaksDocument26 pagesInvestigating OutbreaksSaad Motawéa50% (2)
- GM 05 TrypanosomDocument30 pagesGM 05 TrypanosomSaad MotawéaNo ratings yet
- Julian Pe ToDocument41 pagesJulian Pe ToSaad MotawéaNo ratings yet
- Public Health Community Preparedness For SarsDocument29 pagesPublic Health Community Preparedness For SarsSaad MotawéaNo ratings yet
- Parasites LectureDocument22 pagesParasites LectureSaad MotawéaNo ratings yet
- Pathogenomic Research in Hungary: Present Stage and PerspectivesDocument11 pagesPathogenomic Research in Hungary: Present Stage and PerspectivesSaad MotawéaNo ratings yet
- Case 2Document20 pagesCase 2Saad MotawéaNo ratings yet
- Common Intertinal Worms Found in Southern AfricaDocument100 pagesCommon Intertinal Worms Found in Southern AfricaSaad MotawéaNo ratings yet
- Paraneoplastic SyndromeDocument1 pageParaneoplastic SyndromeSaad MotawéaNo ratings yet
- New York University School of Medicine Meeting of The Curriculum CommitteeDocument2 pagesNew York University School of Medicine Meeting of The Curriculum CommitteeSaad MotawéaNo ratings yet
- EpidemiologyDocument7 pagesEpidemiologySaad MotawéaNo ratings yet
- The Bizarre Claims of Hulda ClarkDocument16 pagesThe Bizarre Claims of Hulda ClarkSaad Motawéa100% (1)
- A Cute Appendic ItsDocument109 pagesA Cute Appendic ItsYosevine Noviana PeranginanginNo ratings yet
- S P - O F: Yllabus RE Rder ORMDocument1 pageS P - O F: Yllabus RE Rder ORMSaad MotawéaNo ratings yet
- CasesDocument18 pagesCasesSaad MotawéaNo ratings yet
- Annual Report 2005 PDFDocument54 pagesAnnual Report 2005 PDFSaad MotawéaNo ratings yet
- Hexamine Fuel TabletDocument4 pagesHexamine Fuel TabletSaad MotawéaNo ratings yet
- GuideDocument41 pagesGuideSaad MotawéaNo ratings yet
- Courses2006 2007Document8 pagesCourses2006 2007Saad MotawéaNo ratings yet
- ApplicationDocument11 pagesApplicationSaad MotawéaNo ratings yet
- Supportive SupervisionDocument21 pagesSupportive SupervisionSaad MotawéaNo ratings yet
- Writing A ReferenceDocument1 pageWriting A ReferenceSaad MotawéaNo ratings yet
- Referral for Suspected Ectopic PregnancyDocument19 pagesReferral for Suspected Ectopic PregnancynjNo ratings yet
- Medical Biology 3Document42 pagesMedical Biology 3Malik MohamedNo ratings yet
- Nclex Study GuideDocument35 pagesNclex Study Guiderachel94% (115)
- Abdominal TraumaDocument52 pagesAbdominal TraumaDONALD UNASHENo ratings yet
- Basic ECG Interpretation 20-Question Practice TestDocument7 pagesBasic ECG Interpretation 20-Question Practice Testemmaaziz100% (1)
- BSN 3F 2B Ectopic Pregnancy PIH Case PresDocument47 pagesBSN 3F 2B Ectopic Pregnancy PIH Case PresKenji ToleroNo ratings yet
- NeoplasiaDocument13 pagesNeoplasiaTisha GrandeNo ratings yet
- Deficient Fluid Volume (Isotonic) : Anxiety FearDocument2 pagesDeficient Fluid Volume (Isotonic) : Anxiety FearVincent Paul SantosNo ratings yet
- Differential Diagnosis Of Autism Spectrum Disorder Katherine K M Stavropoulos full chapterDocument41 pagesDifferential Diagnosis Of Autism Spectrum Disorder Katherine K M Stavropoulos full chapterscott.villalobos894100% (5)
- Scleroderma: Quick Recertific Ation SeriesDocument2 pagesScleroderma: Quick Recertific Ation SeriesvieeveeNo ratings yet
- Leg Ulcer, What Do You Stand byDocument2 pagesLeg Ulcer, What Do You Stand byFree PizzaNo ratings yet
- Colegio de San Juan de Letran: College of Liberal Arts and SciencesDocument7 pagesColegio de San Juan de Letran: College of Liberal Arts and SciencesMaria Elena AquinoNo ratings yet
- Lasercyte DX Dot Plot Poster enDocument2 pagesLasercyte DX Dot Plot Poster enSpital Veterinar AndivetNo ratings yet
- Use of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyDocument5 pagesUse of The Mini International Neuropsychiatric Interview (MINI) As A Screening Tool in Prisons: Results of A Preliminary StudyRafael MartinsNo ratings yet
- Common Cold Remedies Under 40 CharactersDocument541 pagesCommon Cold Remedies Under 40 CharactersMahesh JayaramanNo ratings yet
- Case Study PneumoniaDocument8 pagesCase Study PneumoniaThesa FedericoNo ratings yet
- Septic ArthritisDocument21 pagesSeptic ArthritisDawex IsraelNo ratings yet
- HF GuidelinesDocument76 pagesHF GuidelinesLinto JohnNo ratings yet
- Uncovering Haemophilus: Characteristics, Diagnosis and TreatmentDocument16 pagesUncovering Haemophilus: Characteristics, Diagnosis and TreatmentUSI - GENIO, EMMANUEL JOHNNo ratings yet
- Protein Energy MalnutritionDocument24 pagesProtein Energy Malnutritionapi-312933466100% (1)
- Sideroblastic Anemia Guide: Causes, Symptoms & TypesDocument18 pagesSideroblastic Anemia Guide: Causes, Symptoms & TypesSonam Joshi100% (2)
- Transferring and BandagingDocument8 pagesTransferring and BandagingDarwin AndalNo ratings yet
- TPT Talking Points BookletDocument9 pagesTPT Talking Points BookletNasasira BensonNo ratings yet
- Pleural PathologiesDocument34 pagesPleural PathologiesAshwani RamawatNo ratings yet
- Krok 1 Stomatology 2012Document22 pagesKrok 1 Stomatology 2012Saaha ParmarNo ratings yet
- Swine FluDocument8 pagesSwine Flumohammadomerkhan96No ratings yet
- Blood 2013 Gernsheimer 38 47Document11 pagesBlood 2013 Gernsheimer 38 47Nur Rahmat WibowoNo ratings yet
- Final DraftDocument2 pagesFinal Draftapi-444157113No ratings yet
- Articulo Manejo Paciente IrcDocument8 pagesArticulo Manejo Paciente IrcJUAN FONSECANo ratings yet
- Data e Prezentimit 07/04/2023: Nr. Dosja Studenti Tema: Plani I Kujdesit Infermieror Tek Pacienti Me "Document46 pagesData e Prezentimit 07/04/2023: Nr. Dosja Studenti Tema: Plani I Kujdesit Infermieror Tek Pacienti Me "Gabriela MrijajNo ratings yet