You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- UV-2401-2501PC IM UsersSystemGuide RevCocrDocument65 pagesUV-2401-2501PC IM UsersSystemGuide RevCocrAisha Mutiara100% (1)
- E7d61 139.new Directions in Race Ethnicity and CrimeDocument208 pagesE7d61 139.new Directions in Race Ethnicity and CrimeFlia Rincon Garcia SoyGabyNo ratings yet
- Bring Your Gear 2010: Safely, Easily and in StyleDocument76 pagesBring Your Gear 2010: Safely, Easily and in StyleAkoumpakoula TampaoulatoumpaNo ratings yet
- Jurnal AgusDocument5 pagesJurnal AgusAisha MutiaraNo ratings yet
- Orthopedic Traction of The Maxilla With Miniplates, A New Perspective For Treatment of Midface DeficiencyDocument11 pagesOrthopedic Traction of The Maxilla With Miniplates, A New Perspective For Treatment of Midface DeficiencyAisha MutiaraNo ratings yet
- Tgs Terstruktur GajiDocument8 pagesTgs Terstruktur GajiAisha MutiaraNo ratings yet
- Ethics, Employee Rights, and Employer ResponsibilitiesDocument20 pagesEthics, Employee Rights, and Employer ResponsibilitiesAisha Mutiara100% (1)
- Lamp IranDocument6 pagesLamp IranAisha MutiaraNo ratings yet
- Case Report Resin-Bonded Bridge: Conservative Treatment Option For Single Tooth ReplacementDocument5 pagesCase Report Resin-Bonded Bridge: Conservative Treatment Option For Single Tooth ReplacementAisha MutiaraNo ratings yet
- GTC 8 - PONTICS (PPSG Lectures)Document10 pagesGTC 8 - PONTICS (PPSG Lectures)Aisha MutiaraNo ratings yet
- Sigma Quick Instruction EU1Document2 pagesSigma Quick Instruction EU1Aisha MutiaraNo ratings yet
- Science of Thought and EthicsDocument27 pagesScience of Thought and EthicsAisha MutiaraNo ratings yet
- Solare Ifu Asia 100302dkDocument1 pageSolare Ifu Asia 100302dkAisha MutiaraNo ratings yet
- GTC 4 - Impressions & Retraction Cord (PPSG Lectures)Document34 pagesGTC 4 - Impressions & Retraction Cord (PPSG Lectures)Aisha MutiaraNo ratings yet
- Bahan SGDDocument54 pagesBahan SGDAisha MutiaraNo ratings yet
- GTC 6 - FINISHING (PPSG Lectures)Document20 pagesGTC 6 - FINISHING (PPSG Lectures)Aisha MutiaraNo ratings yet
- GTC 8 - PONTICS (PPSG Lectures)Document10 pagesGTC 8 - PONTICS (PPSG Lectures)Aisha MutiaraNo ratings yet
- Effect of Fluoride-Containing Bleaching Agents On Bovine Enamel MicrohardnessDocument6 pagesEffect of Fluoride-Containing Bleaching Agents On Bovine Enamel MicrohardnessAisha MutiaraNo ratings yet
- "Tell Me and I Forget, Teach Me and I May Remember, Involve MeDocument1 page"Tell Me and I Forget, Teach Me and I May Remember, Involve MeBesufkad Yalew YihunNo ratings yet
- Configuration Guide - Interface Management (V300R007C00 - 02)Document117 pagesConfiguration Guide - Interface Management (V300R007C00 - 02)Dikdik PribadiNo ratings yet
- Bridge Over BrahmaputraDocument38 pagesBridge Over BrahmaputraRahul DevNo ratings yet
- Stress Management HandoutsDocument3 pagesStress Management HandoutsUsha SharmaNo ratings yet
- "Organized Crime" and "Organized Crime": Indeterminate Problems of Definition. Hagan Frank E.Document12 pages"Organized Crime" and "Organized Crime": Indeterminate Problems of Definition. Hagan Frank E.Gaston AvilaNo ratings yet
- Job Satisfaction of Library Professionals in Maharashtra State, India Vs ASHA Job Satisfaction Scale: An Evaluative Study Dr. Suresh JangeDocument16 pagesJob Satisfaction of Library Professionals in Maharashtra State, India Vs ASHA Job Satisfaction Scale: An Evaluative Study Dr. Suresh JangeNaveen KumarNo ratings yet
- School Based Management Contextualized Self Assessment and Validation Tool Region 3Document29 pagesSchool Based Management Contextualized Self Assessment and Validation Tool Region 3Felisa AndamonNo ratings yet
- L GSR ChartsDocument16 pagesL GSR ChartsEmerald GrNo ratings yet
- Chapter 01 What Is Statistics?Document18 pagesChapter 01 What Is Statistics?windyuriNo ratings yet
- Nominal GroupDocument3 pagesNominal GroupSrourNo ratings yet
- Halloween EssayDocument2 pagesHalloween EssayJonathan LamNo ratings yet
- CE EVALUATION EXAM No. 4 - MGT, Fluid Properties, Hydrostatic Force (Answer Key)Document6 pagesCE EVALUATION EXAM No. 4 - MGT, Fluid Properties, Hydrostatic Force (Answer Key)Angelice Alliah De la CruzNo ratings yet
- Moral GPS: A Positive Ethic For Our Multicultural WorldDocument279 pagesMoral GPS: A Positive Ethic For Our Multicultural WorldLeonard Bowman75% (4)
- TM Mic Opmaint EngDocument186 pagesTM Mic Opmaint Engkisedi2001100% (2)
- Source:: APJMR-Socio-Economic-Impact-of-Business-Establishments - PDF (Lpubatangas - Edu.ph)Document2 pagesSource:: APJMR-Socio-Economic-Impact-of-Business-Establishments - PDF (Lpubatangas - Edu.ph)Ian EncarnacionNo ratings yet
- 123Document3 pages123Phoebe AradoNo ratings yet
- Determinant of Nurses' Response Time in Emergency Department When Taking Care of A PatientDocument9 pagesDeterminant of Nurses' Response Time in Emergency Department When Taking Care of A PatientRuly AryaNo ratings yet
- Scrum Exam SampleDocument8 pagesScrum Exam SampleUdhayaNo ratings yet
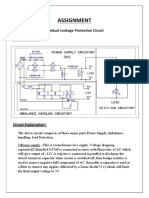
- Assignment: Residual Leakage Protection Circuit Circuit DiagramDocument2 pagesAssignment: Residual Leakage Protection Circuit Circuit DiagramShivam ShrivastavaNo ratings yet
- Jinivefsiti: Sultan LorisDocument13 pagesJinivefsiti: Sultan LorisSITI HAJAR BINTI MOHD LATEPINo ratings yet
- Meta100 AP Brochure WebDocument15 pagesMeta100 AP Brochure WebFirman RamdhaniNo ratings yet
- MPI Unit 4Document155 pagesMPI Unit 4Dishant RathiNo ratings yet
- A202 KBK3043 - Assignment Individual (20%) Review LiteratureDocument5 pagesA202 KBK3043 - Assignment Individual (20%) Review LiteratureAlfie AliNo ratings yet
- SDS ERSA Rev 0Document156 pagesSDS ERSA Rev 0EdgarVelosoCastroNo ratings yet
- CPD - SampleDocument3 pagesCPD - SampleLe Anh DungNo ratings yet
- Cameron International Corporation: FORM 10-KDocument31 pagesCameron International Corporation: FORM 10-KMehdi SoltaniNo ratings yet
- CIPD L5 EML LOL Wk3 v1.1Document19 pagesCIPD L5 EML LOL Wk3 v1.1JulianNo ratings yet
- Title: Smart Monitoring & Control of Electrical Distribution System Using IOTDocument27 pagesTitle: Smart Monitoring & Control of Electrical Distribution System Using IOTwaleed HaroonNo ratings yet