You might also like
- Metabolic Encephalopathies and Delirium: Panayiotis N. Varelas, MD, PHDDocument34 pagesMetabolic Encephalopathies and Delirium: Panayiotis N. Varelas, MD, PHDjorge_suoNo ratings yet
- Delirium: DefenitionDocument18 pagesDelirium: DefenitionNanda MaulanaNo ratings yet
- Huntington’s Chorea, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHuntington’s Chorea, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 1 out of 5 stars1/5 (1)
- Guillain Barre SyndromeDocument19 pagesGuillain Barre SyndromeCrisMartAgullanaNo ratings yet
- Errors of The Proline and Serine MetabolismDocument29 pagesErrors of The Proline and Serine MetabolismHannah CokerNo ratings yet
- Nbme 28 ADocument200 pagesNbme 28 Asabrina kawkabNo ratings yet
- Canine Hypoadrenocorticism Overvew Diagnosis and Treatment LolattiDocument6 pagesCanine Hypoadrenocorticism Overvew Diagnosis and Treatment LolattiAna Clara SevasteNo ratings yet
- Peripheral Neuropathy Diff Diagnosis and Management AafpDocument6 pagesPeripheral Neuropathy Diff Diagnosis and Management Aafpgus_lions100% (1)
- Urine Screening For Metabolic Disorders: Learning ObjectivesDocument12 pagesUrine Screening For Metabolic Disorders: Learning ObjectivesJonalyn LumantasNo ratings yet
- Neonatal Seizures: Postgraduate Dept of PediatricsDocument42 pagesNeonatal Seizures: Postgraduate Dept of PediatricsG VenkateshNo ratings yet
- Descending ParalysisDocument7 pagesDescending ParalysisgianpinotNo ratings yet
- Hartnup's DiseaseDocument20 pagesHartnup's DiseaseAradhanaRamchandani0% (2)
- Wikipedia: 3.1.-Una Patologia On Està Implicada. Modificació Estructural I Funcional (100 Paraules) (Jose)Document4 pagesWikipedia: 3.1.-Una Patologia On Està Implicada. Modificació Estructural I Funcional (100 Paraules) (Jose)jcasanovas1995No ratings yet
- 22 MetabolicEncephalopathies FinalDocument19 pages22 MetabolicEncephalopathies FinalShravan BimanapalliNo ratings yet
- Narcolepsy: Clinical Features, Co-Morbidities & Treatment: Review ArticleDocument12 pagesNarcolepsy: Clinical Features, Co-Morbidities & Treatment: Review ArticlebobyNo ratings yet
- (03241750 - Acta Medica Bulgarica) Recurrent Hyponatremia As Presenting Manifestation of Pituitary MacroadenomaDocument4 pages(03241750 - Acta Medica Bulgarica) Recurrent Hyponatremia As Presenting Manifestation of Pituitary MacroadenomaTeodorNo ratings yet
- Inborn Errors of Amino Acid Metabolism: (Advanced Nutrition)Document8 pagesInborn Errors of Amino Acid Metabolism: (Advanced Nutrition)Deepshikha PatelNo ratings yet
- Wernicke Encephalopathy: EtiologyDocument6 pagesWernicke Encephalopathy: EtiologyDrhikmatullah SheraniNo ratings yet
- Pharmacology Case StudyDocument2 pagesPharmacology Case StudyAntonio CharismaNo ratings yet
- 32 IndianDocument3 pages32 IndianPrateek Kumar PandaNo ratings yet
- KULMAN - 2000 Evidence of Pineal Endocrine Hypofunction in Autistic ChildrenDocument4 pagesKULMAN - 2000 Evidence of Pineal Endocrine Hypofunction in Autistic ChildrenErika PratistaNo ratings yet
- Biochemistry - METABOLISM OF PROTEINDocument44 pagesBiochemistry - METABOLISM OF PROTEINrebeccaNo ratings yet
- Convulsive Disorder: Name: Patel Diya Roll No: 25 Subject: Child Health NursingDocument21 pagesConvulsive Disorder: Name: Patel Diya Roll No: 25 Subject: Child Health NursingDiya PatelNo ratings yet
- Schizophrenia: DR - RahmanDocument17 pagesSchizophrenia: DR - RahmanPineappleNo ratings yet
- Lo Week 5 TropmedDocument25 pagesLo Week 5 TropmedDapot SianiparNo ratings yet
- Lo Week 5 TropmedDocument21 pagesLo Week 5 TropmedAnne MeilynNo ratings yet
- Case ScenarioDocument2 pagesCase ScenarioKityre Maldecir SilvestreNo ratings yet
- Orphanet Journal of Rare DiseasesDocument10 pagesOrphanet Journal of Rare DiseasesIsabela Elena CretuNo ratings yet
- Management of Perinatal AsphyxiaDocument4 pagesManagement of Perinatal AsphyxiaBharath Reddy DNo ratings yet
- Sindrom ChoreaDocument12 pagesSindrom ChoreamolenNo ratings yet
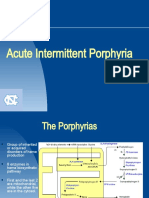
- 12.7.07 AIP GoldenDocument16 pages12.7.07 AIP Goldensshanze12No ratings yet
- Fenilketonuria: Devi WuysangDocument23 pagesFenilketonuria: Devi WuysangChristantina Pradescha AssaNo ratings yet
- Addison Disease: Diagnosis and Initial ManagementDocument5 pagesAddison Disease: Diagnosis and Initial ManagementI Gede SubagiaNo ratings yet
- Journal - Toxic Optic NeuropathyDocument16 pagesJournal - Toxic Optic NeuropathyGisniLuthviatulNo ratings yet
- Poisoning and Drug OverdosageDocument70 pagesPoisoning and Drug Overdosagenathan asfahaNo ratings yet
- Pituitary &thyroid NotesDocument7 pagesPituitary &thyroid NotesAli salimNo ratings yet
- Neonatal Seizures: Chairperson - Prof A K Datta Speaker - Dr. SoutrikDocument21 pagesNeonatal Seizures: Chairperson - Prof A K Datta Speaker - Dr. SoutrikbidisNo ratings yet
- Syndrome of Inappropriate Antidiuretic Hormone Secretion: A Story of Duloxetine-Induced HyponatraemiaDocument3 pagesSyndrome of Inappropriate Antidiuretic Hormone Secretion: A Story of Duloxetine-Induced HyponatraemiaMark Vertiz CernaNo ratings yet
- Niemann Pick DiseaseDocument3 pagesNiemann Pick Diseaseडा. सत्यदेव त्यागी आर्यNo ratings yet
- Absans, MiklonikDocument11 pagesAbsans, MiklonikrendyNo ratings yet
- 167 321 1 PB PDFDocument6 pages167 321 1 PB PDFNorma YantiNo ratings yet
- Thyrotoxic Periodic Paralysis As A Presentation of Thyrotoxicosis: A Case ReportDocument4 pagesThyrotoxic Periodic Paralysis As A Presentation of Thyrotoxicosis: A Case ReportAdvanced Research PublicationsNo ratings yet
- BotulismDocument7 pagesBotulismAmmar AsolyNo ratings yet
- Urea Cycle Disorders: Moderator: Dr. A.K Bala Speaker: Dr. Aradhana MishraDocument28 pagesUrea Cycle Disorders: Moderator: Dr. A.K Bala Speaker: Dr. Aradhana MishraIndranil DuttaNo ratings yet
- Swaiman 99Document34 pagesSwaiman 99Van John MagallanesNo ratings yet
- Organophosphrous PoisoningDocument53 pagesOrganophosphrous Poisoningpriyashu78100% (1)
- 27 June Thyroid Disorders Face To Face Handout P1Document115 pages27 June Thyroid Disorders Face To Face Handout P1Mia DangaNo ratings yet
- Hartnup Disease - Causes, Symptoms & DiagnosisDocument3 pagesHartnup Disease - Causes, Symptoms & DiagnosisYunistya Dwi Cahyani100% (1)
- ng00229 PDFDocument3 pagesng00229 PDFPaijo SusenoNo ratings yet
- MRCP 1 On Examination OGDocument23 pagesMRCP 1 On Examination OGCherryNo ratings yet
- Toxin-Inducedacute Delirium: Alice Cai,, Xuemei CaiDocument18 pagesToxin-Inducedacute Delirium: Alice Cai,, Xuemei CaiVivi DeviyanaNo ratings yet
- Orina Verde en PropofolDocument3 pagesOrina Verde en PropofolEsteban De León ChiNo ratings yet
- Fulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakyDocument108 pagesFulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakypadmaNo ratings yet
- Addison Disease: Diagnosis and Initial ManagementDocument4 pagesAddison Disease: Diagnosis and Initial ManagementTeguh RahNo ratings yet
- PBL WEEK 5 - SCDocument10 pagesPBL WEEK 5 - SCJesselyn ReginaNo ratings yet
- 2.4.4.3D Reye's Syndrome - Dr. SaptinoDocument48 pages2.4.4.3D Reye's Syndrome - Dr. Saptinonawal asmadiNo ratings yet
- PARKINSONISMDocument5 pagesPARKINSONISMPrashanth RajuNo ratings yet
- A Case Report On Hyponatremia Leading Sign of Hypopituitarism (Secondary To Adrenal Insufficiency)Document4 pagesA Case Report On Hyponatremia Leading Sign of Hypopituitarism (Secondary To Adrenal Insufficiency)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Central Pontine Myelinolysis and The Osmotic Demyelination 2021Document10 pagesCentral Pontine Myelinolysis and The Osmotic Demyelination 2021Nicolas RodriguezNo ratings yet
- Background: Emedicine Specialties Psychiatry EmergencyDocument20 pagesBackground: Emedicine Specialties Psychiatry EmergencyStanley Wu TaiNo ratings yet
- Herbal Treatment of Parkinsonism A ReviewDocument7 pagesHerbal Treatment of Parkinsonism A ReviewKartika BorraNo ratings yet
- EINCbrochure - Sept2011 No FoorprintingDocument12 pagesEINCbrochure - Sept2011 No FoorprintingAraChanchiRamchandaniNo ratings yet
- The Critical Care Nurse's Role in EOLDocument9 pagesThe Critical Care Nurse's Role in EOLGemgem Acosta0% (1)
- Energy Protein: Dramatic Changes in Growth and Development To Support, Appropriate Balance of All Nutrients EssentialDocument4 pagesEnergy Protein: Dramatic Changes in Growth and Development To Support, Appropriate Balance of All Nutrients EssentialAraChanchiRamchandaniNo ratings yet
- Nursing HistoryDocument1 pageNursing HistoryAraChanchiRamchandaniNo ratings yet
- Head To ToeDocument2 pagesHead To ToeAraChanchiRamchandaniNo ratings yet
- Supilanas, Ivy Keith R. FEBRUARY 5, 2016 Bsmt-3F Sir Roderick BalceDocument9 pagesSupilanas, Ivy Keith R. FEBRUARY 5, 2016 Bsmt-3F Sir Roderick Balcecoleen paraynoNo ratings yet
- Medical Oneliners SampleDocument5 pagesMedical Oneliners SamplemedpgnotesNo ratings yet
- 020 - Metabolism of Proteins 3Document12 pages020 - Metabolism of Proteins 3Sargonan RaviNo ratings yet
- Hartnup's DiseaseDocument20 pagesHartnup's DiseaseAraChanchiRamchandaniNo ratings yet
- AIIMS May 2017 PDFDocument32 pagesAIIMS May 2017 PDFStelaWatsonNo ratings yet
- Rems FM Shelf May 2022Document80 pagesRems FM Shelf May 2022Manthan PatelNo ratings yet
- Pellagra ArticleDocument11 pagesPellagra ArticleKhylamarie VillalunaNo ratings yet
- Hartnup Disease - Causes, Symptoms & DiagnosisDocument3 pagesHartnup Disease - Causes, Symptoms & DiagnosisYunistya Dwi Cahyani100% (1)
- Urinalysis 2Document9 pagesUrinalysis 2Dawn GonzagaNo ratings yet
- Inborn Errors of Amino Acid MetabolismDocument65 pagesInborn Errors of Amino Acid MetabolismSantino MajokNo ratings yet
- Urine Screening For Metabolic DisordersDocument9 pagesUrine Screening For Metabolic DisordersXyleene Jency Bien IINo ratings yet
- Overview of Water-Soluble VitaminsDocument32 pagesOverview of Water-Soluble VitaminsJames Cojab SacalNo ratings yet
- Amino Acid Metabolism All LecturesDocument18 pagesAmino Acid Metabolism All Lecturesmizare29gNo ratings yet
- 1 Overview & DigestionAbsorption Protein MetabolismDocument37 pages1 Overview & DigestionAbsorption Protein MetabolismAshish K JoyNo ratings yet
- Q.P. CODE:500-A-OR: BiochemistryDocument38 pagesQ.P. CODE:500-A-OR: BiochemistrySai KiranNo ratings yet
- 11-01 Amino Acids - Nitrogen DisposalDocument53 pages11-01 Amino Acids - Nitrogen DisposalFrankenstein MelancholyNo ratings yet