You might also like
- Scared SickDocument320 pagesScared SickChapali100% (5)
- Understanding Delirium: Causes, Symptoms, and TreatmentDocument26 pagesUnderstanding Delirium: Causes, Symptoms, and TreatmentAnkush Sharma100% (1)
- Delirium: DefenitionDocument18 pagesDelirium: DefenitionNanda MaulanaNo ratings yet
- Speciality: General Medicine Case: Nephrotic Syndrome HistoryDocument49 pagesSpeciality: General Medicine Case: Nephrotic Syndrome Historydrtpk100% (2)
- Dementia & DeliriumDocument170 pagesDementia & Deliriummengaku0% (1)
- Oral Tumor / Cancer: Wirsma Arif Harahap Head Neck and Breast Oncology Consultant Andalas Medical School PadangDocument55 pagesOral Tumor / Cancer: Wirsma Arif Harahap Head Neck and Breast Oncology Consultant Andalas Medical School Padangnawal asmadiNo ratings yet
- Hepatic Encephalopathy and ComaDocument19 pagesHepatic Encephalopathy and ComaJas Castro JoveroNo ratings yet
- DeliriumDocument45 pagesDeliriumEhab KhiryNo ratings yet
- Case Study on Seizure DisorderDocument6 pagesCase Study on Seizure DisorderELaine ELena TiongsonNo ratings yet
- Guillain Barre SyndromeDocument19 pagesGuillain Barre SyndromeCrisMartAgullanaNo ratings yet
- Q: Describe The Diagnostic Criteria & Lab Investigation of SLE. AnsDocument28 pagesQ: Describe The Diagnostic Criteria & Lab Investigation of SLE. AnsSajib Nakib100% (1)
- Lyme Disease and Tick-Born Co-Infections: Emily Maiella N.D. Montague Integrative Health 413.230.4462Document79 pagesLyme Disease and Tick-Born Co-Infections: Emily Maiella N.D. Montague Integrative Health 413.230.4462Manasi PalavNo ratings yet
- Ipcr Accomplishment June To Dec 2020Document3 pagesIpcr Accomplishment June To Dec 2020edwardraymond holl0% (1)
- Ketorolac (Drug Study)Document2 pagesKetorolac (Drug Study)Cassandra Grace Labial Paynter89% (18)
- Flower EsscencesDocument2 pagesFlower EsscencesDivyajyoti DevaNo ratings yet
- Management of Unconscious PatientDocument51 pagesManagement of Unconscious PatientEmenike Donald Ejieji50% (2)
- Delirium and Its ManagmentDocument64 pagesDelirium and Its ManagmentViren Solanki100% (1)
- DeliriumDocument27 pagesDeliriumBushra EjazNo ratings yet
- Neonatal Seizures: - Dr.C.S.N.VittalDocument23 pagesNeonatal Seizures: - Dr.C.S.N.VittalRidanna HartateanaNo ratings yet
- Epidemiology of BPVC Clinical Features of BPVC: Gen Med C Presents . Benign Paroxysmal Vertigo of Childhood (BPVC)Document5 pagesEpidemiology of BPVC Clinical Features of BPVC: Gen Med C Presents . Benign Paroxysmal Vertigo of Childhood (BPVC)laureeateNo ratings yet
- Reye and Reye-Like Syndromes: DR / Reyad AlfakyDocument59 pagesReye and Reye-Like Syndromes: DR / Reyad AlfakyMegan N. ReyesNo ratings yet
- Fulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakyDocument108 pagesFulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakypadmaNo ratings yet
- Reye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocument7 pagesReye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreeNo ratings yet
- Reye's SyndromeDocument8 pagesReye's SyndromeRadhiatul AdillahNo ratings yet
- DeliriumDocument40 pagesDeliriumAklile TsegaNo ratings yet
- Approach To Comatose Child: DR G.VenkateshDocument83 pagesApproach To Comatose Child: DR G.VenkateshG VenkateshNo ratings yet
- Family Med Collector PDFDocument9 pagesFamily Med Collector PDFMohammedNo ratings yet
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathypraveenbhavniNo ratings yet
- Case No. 6 Lost The PlotDocument7 pagesCase No. 6 Lost The PlotNermeen AlrajhiNo ratings yet
- Wernicke Encephalopathy: EtiologyDocument6 pagesWernicke Encephalopathy: EtiologyDrhikmatullah SheraniNo ratings yet
- Unconscious Child AssessmentDocument52 pagesUnconscious Child Assessmentar bindraNo ratings yet
- Niemann Pick DiseaseDocument3 pagesNiemann Pick Diseaseडा. सत्यदेव त्यागी आर्यNo ratings yet
- Clinical Features A) Upper Urinary Tract (Pyelonephritis) :: T:Marwa AL-Headri 1Document16 pagesClinical Features A) Upper Urinary Tract (Pyelonephritis) :: T:Marwa AL-Headri 1abnaltag667No ratings yet
- Neurologic DiseasesDocument13 pagesNeurologic DiseasesCzarinah BacuadoNo ratings yet
- Acute EncephalopathyDocument4 pagesAcute Encephalopathymadimadi11No ratings yet
- Organic Mental DisorderDocument40 pagesOrganic Mental DisorderSumam NeveenNo ratings yet
- DeliriumDocument15 pagesDeliriumSulieman MazahrehNo ratings yet
- Delirium (JC)Document28 pagesDelirium (JC)hillary temboNo ratings yet
- Boyantin ArticleDocument5 pagesBoyantin ArticleVivekNo ratings yet
- Delirium & Assessing A Confused Patient: CriteriaDocument9 pagesDelirium & Assessing A Confused Patient: CriteriaDeedz01No ratings yet
- Neurocognitive Disorders by Hiwot G. (BSC, MSC)Document113 pagesNeurocognitive Disorders by Hiwot G. (BSC, MSC)girmaw yidegNo ratings yet
- Acute Liver FailureDocument69 pagesAcute Liver FailureAsif.N.IqbalNo ratings yet
- Causes, Assessment and Management of ComaDocument30 pagesCauses, Assessment and Management of ComaDrGasnasNo ratings yet
- Detect and Treat Agitated Delirium QuicklyDocument54 pagesDetect and Treat Agitated Delirium QuicklyVishwa ReddyNo ratings yet
- Convulsive Disorder: Name: Patel Diya Roll No: 25 Subject: Child Health NursingDocument21 pagesConvulsive Disorder: Name: Patel Diya Roll No: 25 Subject: Child Health NursingDiya PatelNo ratings yet
- Autoimmune Polyglandular Syndrome ReviewDocument3 pagesAutoimmune Polyglandular Syndrome ReviewIan AlvaradoNo ratings yet
- Quiz Blessings #6Document7 pagesQuiz Blessings #6Rachel LiuNo ratings yet
- Case Study Dandy2Document24 pagesCase Study Dandy2lolo223100% (1)
- Coma-Causes, Diagnosis, Treatment and ManagementDocument19 pagesComa-Causes, Diagnosis, Treatment and ManagementHabtamu AdimasuNo ratings yet
- DELIRIUMDocument68 pagesDELIRIUMVarada PanikkathNo ratings yet
- Type 1 Diabetes Mellitus PP pth617Document10 pagesType 1 Diabetes Mellitus PP pth617api-621438645No ratings yet
- Reversible Dementia and DeliriumDocument65 pagesReversible Dementia and Deliriummpm8471No ratings yet
- Referral Guide Lines For Patient With HeadacheDocument13 pagesReferral Guide Lines For Patient With HeadacheImad Q. KhaleelNo ratings yet
- Diagnosis of EncephalitisDocument59 pagesDiagnosis of EncephalitisFebrian Indra Jr.No ratings yet
- Pembahasan UKDI CLINIC 3 Batch Mei 2016Document662 pagesPembahasan UKDI CLINIC 3 Batch Mei 2016widi kusumaNo ratings yet
- Pituitary &thyroid NotesDocument7 pagesPituitary &thyroid NotesAli salimNo ratings yet
- acutedisseminatedencephalomyelitis-170316222736Document80 pagesacutedisseminatedencephalomyelitis-170316222736Sri Ram 07No ratings yet
- Neonatal SeizuresDocument22 pagesNeonatal SeizuresKatrin Marcelina SihombingNo ratings yet
- Price: Pediatric Nursing, 10 Edition: Open Book Quizzes Chapter 14: Disorders of The School-Age ChildDocument2 pagesPrice: Pediatric Nursing, 10 Edition: Open Book Quizzes Chapter 14: Disorders of The School-Age ChildmickjagerNo ratings yet
- Thyroiditis and Parathyroid GlandDocument29 pagesThyroiditis and Parathyroid GlandTheoder RobinsonNo ratings yet
- m1 C. Mhango - Eclamptic Patient and ManagementDocument24 pagesm1 C. Mhango - Eclamptic Patient and ManagementAddisNo ratings yet
- Diagnostic Criteria and Types of Hepatorenal Syndrome (HRSDocument2 pagesDiagnostic Criteria and Types of Hepatorenal Syndrome (HRSegrajales101No ratings yet
- Complications MalariaDocument4 pagesComplications MalariaBenny Trisaktyari100% (1)
- The Reye Syndrome Sourcebook: A Concise Guide for Parents and PatientsFrom EverandThe Reye Syndrome Sourcebook: A Concise Guide for Parents and PatientsNo ratings yet
- Treatments For TBDocument10 pagesTreatments For TBnawal asmadiNo ratings yet
- Journal Brain Tumor MRIDocument7 pagesJournal Brain Tumor MRInawal asmadiNo ratings yet
- Diagnosis and Management of Tubo-Ovarian Abscesses: AetiologyDocument9 pagesDiagnosis and Management of Tubo-Ovarian Abscesses: Aetiologyriko janukadriNo ratings yet
- Primary Evaluation and Acute Management of Vertigo.17Document5 pagesPrimary Evaluation and Acute Management of Vertigo.17nawal asmadiNo ratings yet
- Helminth - PictureDocument17 pagesHelminth - Picturenawal asmadiNo ratings yet
- Fome 10Document41 pagesFome 10Sherly Vanessa putriNo ratings yet
- Met - BEt 2018Document33 pagesMet - BEt 2018Imam HamdaNo ratings yet
- KP 1.4.2.7 Heme SynthesisDocument14 pagesKP 1.4.2.7 Heme Synthesisnawal asmadiNo ratings yet
- Virus Replication: John Goulding, Imperial College London, UKDocument1 pageVirus Replication: John Goulding, Imperial College London, UKnawal asmadiNo ratings yet
- Batu Saluran Kemih Etio-Patogenesis PencegahanDocument43 pagesBatu Saluran Kemih Etio-Patogenesis Pencegahanikhlasia AmaliNo ratings yet
- Pediatrik AritmiaDocument27 pagesPediatrik Aritmianawal asmadiNo ratings yet
- 3.1.4.1 Trauma Traktus UrinariusDocument1 page3.1.4.1 Trauma Traktus Urinariusnawal asmadiNo ratings yet
- Jejas Sel dan Inflamasi Patologi AnatomiDocument25 pagesJejas Sel dan Inflamasi Patologi Anatominawal asmadiNo ratings yet
- 2.5.1.6B Kuliah ASDocument30 pages2.5.1.6B Kuliah ASAfifahNo ratings yet
- Treatment of Cardiogenic ShockDocument3 pagesTreatment of Cardiogenic Shocknawal asmadiNo ratings yet
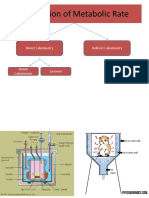
- Calculation of Metabolic RateDocument6 pagesCalculation of Metabolic Ratenawal asmadiNo ratings yet
- Abnormalities in The Digestive SystemDocument2 pagesAbnormalities in The Digestive Systemnawal asmadiNo ratings yet
- Treatments For TBDocument10 pagesTreatments For TBnawal asmadiNo ratings yet
- 10 Tips for Staying Healthy in CollegeDocument3 pages10 Tips for Staying Healthy in Collegenawal asmadiNo ratings yet
- KP 1.5.3.2 - Faktor Yang Mempengaruhi Tumbuh Kenang Janin IntrauterinDocument81 pagesKP 1.5.3.2 - Faktor Yang Mempengaruhi Tumbuh Kenang Janin IntrauterinnadyatulhusnaNo ratings yet
- Heart Failure and Cardiogenic ShockDocument8 pagesHeart Failure and Cardiogenic Shocknawal asmadiNo ratings yet
- 10 Tips for Staying Healthy in CollegeDocument3 pages10 Tips for Staying Healthy in Collegenawal asmadiNo ratings yet
- Penyakit PancreasDocument14 pagesPenyakit Pancreasnawal asmadiNo ratings yet
- Congenital DefectDocument4 pagesCongenital Defectnawal asmadiNo ratings yet
- Pediatrik AritmiaDocument27 pagesPediatrik Aritmianawal asmadiNo ratings yet
- Acute Appendicitis: by Avit SuchitraDocument33 pagesAcute Appendicitis: by Avit Suchitranawal asmadiNo ratings yet
- Tumor Saluran Cerna AtasDocument85 pagesTumor Saluran Cerna Atasnawal asmadiNo ratings yet
- CHILDHOOD DIABETES GUIDEDocument51 pagesCHILDHOOD DIABETES GUIDEnawal asmadiNo ratings yet
- dct1 scenariosDocument14 pagesdct1 scenariosdp2fscgxrxNo ratings yet
- Pharmaceutical Dosage Forms, Drug Delivery Systems and Medical DevicesDocument28 pagesPharmaceutical Dosage Forms, Drug Delivery Systems and Medical Devices陳欣瑩No ratings yet
- STDs-Sexually Transmitted Diseases & Infections GuideDocument11 pagesSTDs-Sexually Transmitted Diseases & Infections GuideYoon Pwint PhyuNo ratings yet
- Angioedema 4Document18 pagesAngioedema 4Venosha GunasekaranNo ratings yet
- IUD Contraception in Dogs TestedDocument4 pagesIUD Contraception in Dogs TestedAristoteles Esteban Cine VelazquezNo ratings yet
- GL On Pertussis Case ManagementDocument32 pagesGL On Pertussis Case Managementnazurah HamidNo ratings yet
- Seminar Electrocardiogram (ECG)Document32 pagesSeminar Electrocardiogram (ECG)Jamuna PatelNo ratings yet
- SNAKE BITE PresentationDocument15 pagesSNAKE BITE Presentationkunnar corrosionNo ratings yet
- Fall Risk Factors For The Learner 1Document13 pagesFall Risk Factors For The Learner 1StokleyCNo ratings yet
- Case: Biopure Corporation: Submitted By-Group 5Document4 pagesCase: Biopure Corporation: Submitted By-Group 5Amba KamatNo ratings yet
- Medical Terminology With Suffixes and PrefixesDocument27 pagesMedical Terminology With Suffixes and PrefixesCrystal Gale TabiosNo ratings yet
- W3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Document22 pagesW3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Rona DindangNo ratings yet
- Robertson2013 PDFDocument88 pagesRobertson2013 PDFArini NurlelaNo ratings yet
- Informed Consent For Lasik SurgeryDocument2 pagesInformed Consent For Lasik SurgeryMoerieda RinquestNo ratings yet
- Teenage Pregnancy Brief DiscussionDocument3 pagesTeenage Pregnancy Brief DiscussionJoanna Peroz100% (1)
- NSW Faculty TRIAL FELLOWSHIP EXAMINATION Short Answer QuestionsDocument42 pagesNSW Faculty TRIAL FELLOWSHIP EXAMINATION Short Answer Questionssacabona50% (2)
- Nursing Impact On Maternal and Infant Mortality in The United States.Document7 pagesNursing Impact On Maternal and Infant Mortality in The United States.boniface mogisoNo ratings yet
- NCP Nephrolithiasis FeverDocument1 pageNCP Nephrolithiasis Feverm_r0se_k0h100% (1)
- DM Foot 81Document20 pagesDM Foot 81Zar Ni OoNo ratings yet
- Hyperosmolar Hyperglycemic StateDocument10 pagesHyperosmolar Hyperglycemic StateMirko S. León RguezNo ratings yet
- STEAM INHALATION and NEBULIZATIONDocument4 pagesSTEAM INHALATION and NEBULIZATIONRenzo GabrielNo ratings yet
- Comparison of ICD-10 and DSM-IV Criteria For Postconcussion SyndromedisorderDocument19 pagesComparison of ICD-10 and DSM-IV Criteria For Postconcussion Syndromedisorderneoraymix blackNo ratings yet
- Feasibility and Efficacy of Home Rectal Irrigation in Neonates and Early Infancy With Hirschsprung DiseaseDocument9 pagesFeasibility and Efficacy of Home Rectal Irrigation in Neonates and Early Infancy With Hirschsprung DiseaseKiki ElvianiNo ratings yet
- Bloodborne Pathogens PPT v-03!01!17Document44 pagesBloodborne Pathogens PPT v-03!01!17kunalphalswal0005No ratings yet
- Fenofibratesimvastatin Fixed-Dose Combination in TDocument13 pagesFenofibratesimvastatin Fixed-Dose Combination in TMade DeanaNo ratings yet