You might also like
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- ESR Basics and AnalyzerDocument39 pagesESR Basics and AnalyzerSmart BiomedicalNo ratings yet
- Tutor Imun HBsAg KuantitatifDocument27 pagesTutor Imun HBsAg Kuantitatifv_mayasari100% (1)
- Should Six Sigma be Calculated for Internal Quality Control in Clinical LaboratoryDocument24 pagesShould Six Sigma be Calculated for Internal Quality Control in Clinical LaboratoryMustakim DuharingNo ratings yet
- Hemostasis Dan Koagulasi: DR - Fedelia Raya, M.Kes, SPPK Bagian Patologi Klinik Fk-UhoDocument18 pagesHemostasis Dan Koagulasi: DR - Fedelia Raya, M.Kes, SPPK Bagian Patologi Klinik Fk-UhoToraoNo ratings yet
- Insert Kit Uji NarkobaDocument2 pagesInsert Kit Uji NarkobaFatimah azzahraNo ratings yet
- Bence Jones Protein-UrineDocument16 pagesBence Jones Protein-UrineDrashua Ashua100% (2)
- Jurnal Gula Darah SewaktuDocument9 pagesJurnal Gula Darah SewaktuIndra TeamRiotNo ratings yet
- Permintaan Pemeriksaan LaboratoriumDocument1 pagePermintaan Pemeriksaan LaboratoriumSMC KRINo ratings yet
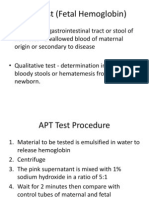
- APT Test (Fetal Hemoglobin)Document11 pagesAPT Test (Fetal Hemoglobin)Diovic TanNo ratings yet
- Infeksi Virus Dengue: Demam Berdarah Dengue Demam DengueDocument62 pagesInfeksi Virus Dengue: Demam Berdarah Dengue Demam DengueMarwi VinaNo ratings yet
- Daftar Nilai Normal Pemeriksaan Laboratorium RsiaDocument4 pagesDaftar Nilai Normal Pemeriksaan Laboratorium Rsialab mutiara bundaNo ratings yet
- Tes Lab Pada Peny Infeksi Dan Tropis (Lebih Singkat)Document71 pagesTes Lab Pada Peny Infeksi Dan Tropis (Lebih Singkat)Monazzt AsshagabNo ratings yet
- Guidelines For The Clinical Management of ThalassemiaDocument205 pagesGuidelines For The Clinical Management of ThalassemiaAmalia Muchammad BafagihNo ratings yet
- Bilirubin Jendrassik-Grof FS Reagent R1 Sulphanilic Acid-Solution - En-GB-17Document9 pagesBilirubin Jendrassik-Grof FS Reagent R1 Sulphanilic Acid-Solution - En-GB-17Rahadian MahargiriNo ratings yet
- Creatinine FS PDFDocument2 pagesCreatinine FS PDFChafa NickNo ratings yet
- EritrositDocument12 pagesEritrositNatasya HerinNo ratings yet
- WBC Disorder PPT 2Document56 pagesWBC Disorder PPT 2YESHASWI PIKLENo ratings yet
- Jurnal Artikel Aau 1 PDFDocument7 pagesJurnal Artikel Aau 1 PDFRizkiSeptiaNo ratings yet
- List of Laboratory Instruments Interfaced: Hematology (Cell Counters)Document2 pagesList of Laboratory Instruments Interfaced: Hematology (Cell Counters)SIMRSNo ratings yet
- CoombsDocument112 pagesCoombsratnadilaNo ratings yet
- Multiple Myeloma OverviewDocument52 pagesMultiple Myeloma OverviewanmegpraNo ratings yet
- Alkaline Phosphatase Activity TestDocument2 pagesAlkaline Phosphatase Activity TestFariz KasyidiNo ratings yet
- P-LCR Parameter - Platelet Large Cell Ratio - Medical LaboratoriesDocument3 pagesP-LCR Parameter - Platelet Large Cell Ratio - Medical LaboratorieshardianNo ratings yet
- Prenatal Screening: HM Sulchan Sofoewan Divisi Feto-Maternal Bagian Obstetri Dan Ginekologi FK UGMDocument54 pagesPrenatal Screening: HM Sulchan Sofoewan Divisi Feto-Maternal Bagian Obstetri Dan Ginekologi FK UGMTahta PambudiNo ratings yet
- Lymphatic Filariasis PDFDocument12 pagesLymphatic Filariasis PDFBai Marifah LucasNo ratings yet
- Bone Marrow Aspiration Guide: Everything You Need to KnowDocument15 pagesBone Marrow Aspiration Guide: Everything You Need to KnowAyu DewiNo ratings yet
- 3-1 - Ida ParwatiDocument34 pages3-1 - Ida ParwatiFaisal NurlanNo ratings yet
- Webinar INAEQAS 27062020. Adhi K. Sugianli, DR., SPPK (K), M.Kes. How To Read The Gram Panel-1Document20 pagesWebinar INAEQAS 27062020. Adhi K. Sugianli, DR., SPPK (K), M.Kes. How To Read The Gram Panel-1Rini WidyantariNo ratings yet
- Para Protein Emi ADocument14 pagesPara Protein Emi AMohamoud MohamedNo ratings yet
- 4.1 Antibodi TrombositDocument36 pages4.1 Antibodi Trombositrani fatinNo ratings yet
- Sindrom Hemolitik UremikDocument24 pagesSindrom Hemolitik UremikLindaaaNo ratings yet
- RFIT-PRT-0895 FilmArrayPneumoplus Instructions For Use EN PDFDocument112 pagesRFIT-PRT-0895 FilmArrayPneumoplus Instructions For Use EN PDFGuneyden GuneydenNo ratings yet
- MMDocument67 pagesMMRatnaNo ratings yet
- Transplantasi Sumsum TulangDocument32 pagesTransplantasi Sumsum TulangSatria Yosi HernawanNo ratings yet
- Bab I-V Jurding Infanticide EditedDocument62 pagesBab I-V Jurding Infanticide EditedS FznsNo ratings yet
- Hematology Reference Values in Indonesian ChildrenDocument16 pagesHematology Reference Values in Indonesian ChildrenRini WidyantariNo ratings yet
- Pemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKDocument16 pagesPemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKZulfan RifqiawanNo ratings yet
- Laboratory Hemostatic DisordersDocument41 pagesLaboratory Hemostatic DisordersYohanna SinuhajiNo ratings yet
- FACSDocument24 pagesFACSMudit MisraNo ratings yet
- Spesifikasi Erba, Hematology Analyzer 3 Part-Diff, Elite 3Document1 pageSpesifikasi Erba, Hematology Analyzer 3 Part-Diff, Elite 3Risqon Anjahiranda AdiputraNo ratings yet
- Monolisa HCV Ag-Ac UltraDocument4 pagesMonolisa HCV Ag-Ac UltraSantiagoAFNo ratings yet
- What'S New in Treatment Monitoring: Viral Load and Cd4 TestingDocument2 pagesWhat'S New in Treatment Monitoring: Viral Load and Cd4 TestingRina ErlinaNo ratings yet
- Pancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseDocument6 pagesPancytopenia As Initial Presentation of Acute Lymphoblastic Leukemia and Its Associationwith Bone MarrowresponseIJAR JOURNALNo ratings yet
- Soal Hematologi 2014Document3 pagesSoal Hematologi 2014Muhammad Faza NaufalNo ratings yet
- DR - Dr. Tri Ratnaningsih, MKes, SPPK (K) - Talasemia Joglo 2021Document20 pagesDR - Dr. Tri Ratnaningsih, MKes, SPPK (K) - Talasemia Joglo 2021Eldo TaufilaNo ratings yet
- Penggunaan Tes Cepat Molekuler Dalam Diagnosis TuberkulosisDocument49 pagesPenggunaan Tes Cepat Molekuler Dalam Diagnosis Tuberkulosishalimah0% (1)
- K4. Diagnosis Holistik - EngDocument21 pagesK4. Diagnosis Holistik - EngBevila KorspoilvilNo ratings yet
- Thalasemia RSCMDocument28 pagesThalasemia RSCMAnonymous ujOv31SNo ratings yet
- Diagnosing Diabetes Insipidus with Dehydration, Water Deprivation, and Desmopressin TestsDocument17 pagesDiagnosing Diabetes Insipidus with Dehydration, Water Deprivation, and Desmopressin TestsM. RamazaliNo ratings yet
- AFPDocument4 pagesAFPHassan GillNo ratings yet
- Dr. Dwi Sunarjadi, MKM Dr. Melania Dessy Savitri Dr. Dwi Sunarjadi, MKM Dr. Melania Dessy SavitriDocument1 pageDr. Dwi Sunarjadi, MKM Dr. Melania Dessy Savitri Dr. Dwi Sunarjadi, MKM Dr. Melania Dessy SavitriMelania Savitri100% (1)
- 1 (2 Files Merged)Document2 pages1 (2 Files Merged)HOTMAIDANo ratings yet
- BrucellosisDocument26 pagesBrucellosisVasilika GiemsaNo ratings yet
- Euis Safarina Perbandingan Kadar Bilirubin Total Pada Serum Segar Dan Serum Simpan 3 Hari Dan 4 Hari Pada Suhu 2-8 CDocument7 pagesEuis Safarina Perbandingan Kadar Bilirubin Total Pada Serum Segar Dan Serum Simpan 3 Hari Dan 4 Hari Pada Suhu 2-8 CHarryNo ratings yet
- BCCA Febrile Neutropenia GuidelinesDocument2 pagesBCCA Febrile Neutropenia GuidelinesdenokayuMRNo ratings yet
- Hormon Paratiroid: Dr. Muniroh, SP - PKDocument10 pagesHormon Paratiroid: Dr. Muniroh, SP - PKFuadi FaisalNo ratings yet
- Problem 3 - VarlaDocument75 pagesProblem 3 - VarlavarlavarleyNo ratings yet
- Understanding Typhoid Fever: Causes, Symptoms and DiagnosisDocument22 pagesUnderstanding Typhoid Fever: Causes, Symptoms and DiagnosisUci MarleyNo ratings yet
- Typhoid Fever: Infectious DiseaseDocument18 pagesTyphoid Fever: Infectious DiseaseSoumyadip PradhanNo ratings yet
- Principal Letter Opposed ImmunizationDocument2 pagesPrincipal Letter Opposed Immunizationmpnaidu13111998100% (1)
- Unidad 2. Tarea 2. EscrituraDocument5 pagesUnidad 2. Tarea 2. EscrituraAndrea ChavarroNo ratings yet
- Ezzat PaperDocument15 pagesEzzat PaperMohamedAbdelmonaemNo ratings yet
- RPS Hospital Ranchi Total Marks - 30 Question Paper Set - 1Document7 pagesRPS Hospital Ranchi Total Marks - 30 Question Paper Set - 1Tanisha Singh100% (1)
- Logbook PSM 2021Document103 pagesLogbook PSM 2021Youtube SubNo ratings yet
- Presentasi Radiologi Edema ParuDocument19 pagesPresentasi Radiologi Edema ParuFia100% (1)
- Spastic Diplegic Cerebral PalsyDocument43 pagesSpastic Diplegic Cerebral PalsyRachel GardnerNo ratings yet
- Jurnal AnestesiDocument5 pagesJurnal AnestesiridwanNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsSanchita KunwerNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Illegal DrugsDocument5 pagesIllegal DrugsJOCELYN VARGASNo ratings yet
- Firm-flaccid penis and erectile dysfunctionDocument12 pagesFirm-flaccid penis and erectile dysfunctionjdelakruz523No ratings yet
- Delivery of Evidence-Based Treatment For Multiple Anxiety Disorders in Primary Care: A Randomized Controlled TrialDocument5 pagesDelivery of Evidence-Based Treatment For Multiple Anxiety Disorders in Primary Care: A Randomized Controlled TrialRaja DarmawanNo ratings yet
- Hospital Standards 2021 - GAHARDocument314 pagesHospital Standards 2021 - GAHARKhalid ElwakilNo ratings yet
- DR Amaefula, E. Temple MBBS, Fwacs, Faoi,: Inflamation, Infection, and Use of Antibiotics in SurgeryDocument40 pagesDR Amaefula, E. Temple MBBS, Fwacs, Faoi,: Inflamation, Infection, and Use of Antibiotics in SurgeryPrincewill SeiyefaNo ratings yet
- Glossary of Patient SafetyDocument352 pagesGlossary of Patient SafetyEman ShalabyNo ratings yet
- Plprevia PDFDocument3 pagesPlprevia PDFAtikah RahmadhaniNo ratings yet
- 340B Drug Discounts WPDocument20 pages340B Drug Discounts WPScott McClallenNo ratings yet
- Clinical Approach To Isolated Splenomegaly: M M, P M, R KDocument5 pagesClinical Approach To Isolated Splenomegaly: M M, P M, R KlilisNo ratings yet
- Professional RNDocument2 pagesProfessional RNapi-121454402No ratings yet
- DulcolaxDocument1 pageDulcolaxKatie McPeekNo ratings yet
- Hip Dislocation ResearchDocument8 pagesHip Dislocation Researchapi-268839011No ratings yet
- Clinical Handover and Patient Safety Literature Review Report 2005Document5 pagesClinical Handover and Patient Safety Literature Review Report 2005gw163ckjNo ratings yet
- In Home ServicesDocument9 pagesIn Home Servicesubertor1234No ratings yet
- Gastro Inter It IsDocument3 pagesGastro Inter It IsDhea Imas WijayantiNo ratings yet
- Femto-Lasik laser eye surgery explainedDocument4 pagesFemto-Lasik laser eye surgery explainedvrlftrNo ratings yet
- Direct Examination of Expert WitnessDocument5 pagesDirect Examination of Expert WitnessRdn Diamante100% (1)
- Cholecystitis - Complications of Cholecystitis A Comprehensive Contemporary Imaging ReviewDocument17 pagesCholecystitis - Complications of Cholecystitis A Comprehensive Contemporary Imaging ReviewSamuel WidjajaNo ratings yet
- Thoracic Surgery: Cervical, Thoracic and Abdominal ApproachesDocument1,068 pagesThoracic Surgery: Cervical, Thoracic and Abdominal ApproachesAlexandru GibuNo ratings yet
- HaemophiliaDocument15 pagesHaemophiliaSanmuga VimalanathanNo ratings yet