You might also like
- Capital Profile - Santosa-Harris Kristanto GozaliDocument9 pagesCapital Profile - Santosa-Harris Kristanto GozalisimplyvenNo ratings yet
- Vascular Diseases (1 of 3)Document4 pagesVascular Diseases (1 of 3)Doctor GeneralNo ratings yet
- Schwartz Chapter 33 SpleenDocument20 pagesSchwartz Chapter 33 SpleenGay Solas Epalan100% (1)
- CHOLEDOCHOLITHIASISDocument38 pagesCHOLEDOCHOLITHIASISPrecious Cofreros100% (3)
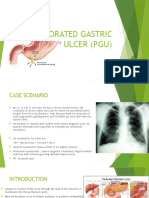
- Perforated Gastric Ulcer (Pgu)Document10 pagesPerforated Gastric Ulcer (Pgu)Jen NeeNo ratings yet
- Colorectal Ca PresentationDocument25 pagesColorectal Ca Presentationapi-399299717No ratings yet
- Oral Histology MCQsDocument27 pagesOral Histology MCQssarah100% (2)
- Minor ConnectorsDocument61 pagesMinor Connectorssarah100% (1)
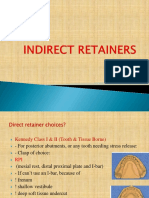
- Indirect RetainersDocument52 pagesIndirect RetainerssarahNo ratings yet
- Indirect RetainersDocument52 pagesIndirect RetainerssarahNo ratings yet
- Thyroid CancerDocument82 pagesThyroid Cancerom100% (1)
- Thyroid CarcinomaDocument27 pagesThyroid CarcinomaGanesh MarutinathNo ratings yet
- Thyroid Cancer PDFDocument67 pagesThyroid Cancer PDFJaredNo ratings yet
- Carcinoma Thyroid: Diagnosis and Management: Professor Ravi KantDocument51 pagesCarcinoma Thyroid: Diagnosis and Management: Professor Ravi KantMubarakDiedaNo ratings yet
- Malignant Tumors of Uterus: DR Tahira RizwanDocument52 pagesMalignant Tumors of Uterus: DR Tahira RizwanSadia YousafNo ratings yet
- Breast Cancer FinalDocument68 pagesBreast Cancer Finalapi-400333454No ratings yet
- Malignant MelanomaDocument31 pagesMalignant MelanomakityamuwesiNo ratings yet
- Ovarian CancerDocument27 pagesOvarian Cancermvs16973100% (1)
- Case Study CA Lower RectumDocument47 pagesCase Study CA Lower RectumArtyom Granovskiy100% (1)
- Antibiotics in SurgeryDocument19 pagesAntibiotics in SurgeryYang JunNo ratings yet
- Powerpoint: Disorders of The Thyroid GlandDocument67 pagesPowerpoint: Disorders of The Thyroid Glandj.doe.hex_87100% (1)
- Surgical Oncology and Breast BiopsyDocument12 pagesSurgical Oncology and Breast Biopsybo gum parkNo ratings yet
- Ca PenisDocument25 pagesCa Penisrajan kumar100% (2)
- Thyroid Carcinoma: DR Suleman Mumtaz PG 2 Ward 2Document81 pagesThyroid Carcinoma: DR Suleman Mumtaz PG 2 Ward 2suleman2009No ratings yet
- 5.surgical Infections LectureDocument56 pages5.surgical Infections LectureBiruk DesalegnNo ratings yet
- Thyroid CancerDocument34 pagesThyroid CancerSahirNo ratings yet
- Carcinoma Penis: Pravin NarkhedeDocument36 pagesCarcinoma Penis: Pravin Narkhedepravin narkhede100% (1)
- December 2013 What Is Necrotizing Fasciitis? What Are Its Causes? How Will You Manage Such A Case?Document3 pagesDecember 2013 What Is Necrotizing Fasciitis? What Are Its Causes? How Will You Manage Such A Case?Vaibhav BharatNo ratings yet
- Prevention & Detection of CANCERDocument32 pagesPrevention & Detection of CANCERSiddharth JainNo ratings yet
- Breast CancerDocument33 pagesBreast Canceredenpearlcastillo67% (3)
- Fat EmbolismDocument12 pagesFat EmbolismHastina HadnanNo ratings yet
- Renal TumorsDocument50 pagesRenal TumorseuromonNo ratings yet
- Colorectal CancerDocument29 pagesColorectal CancerLeeyanBhadzzVagayNo ratings yet
- ThyroidectomyDocument5 pagesThyroidectomyJennelyn LumbreNo ratings yet
- Lip Cancer-Ablative and Reconstructive Surgery: ChapDocument52 pagesLip Cancer-Ablative and Reconstructive Surgery: ChapYang Lin Chen100% (1)
- Renal Trauma: Dr. Mars Dwi Tjahjo, Sp.UDocument21 pagesRenal Trauma: Dr. Mars Dwi Tjahjo, Sp.UbayuNo ratings yet
- 1 CancerpharmacologyDocument121 pages1 Cancerpharmacologydewi100% (1)
- 21 Obstructive JaundiceDocument12 pages21 Obstructive JaundicejumaymayaNo ratings yet
- Acute Leukemia: Thirunavukkarasu MurugappanDocument22 pagesAcute Leukemia: Thirunavukkarasu MurugappanFelix Allen100% (1)
- Cancer Prevention, Screening, & Early DetectionDocument13 pagesCancer Prevention, Screening, & Early Detectionchfalguera100% (1)
- Gyne - Case 15 Benign Lesions of The Vulva & VaginaDocument2 pagesGyne - Case 15 Benign Lesions of The Vulva & Vaginacbac1990No ratings yet
- Vaginal CancerDocument41 pagesVaginal Cancercb_cristianNo ratings yet
- Fluid and Electrolyte Management of The Surgical PatientDocument28 pagesFluid and Electrolyte Management of The Surgical PatientAndri Feisal NasutionNo ratings yet
- Gastrointestinal MalignanciesDocument59 pagesGastrointestinal Malignanciesadamu mohammadNo ratings yet
- Principles of Cancer Management20022013b.Document62 pagesPrinciples of Cancer Management20022013b.Bashiru AminuNo ratings yet
- What Is A Bone Marrow Transplant?Document4 pagesWhat Is A Bone Marrow Transplant?Krisna AgustiniNo ratings yet
- Lung CancerDocument22 pagesLung CancermandrakesMD100% (1)
- Upper Gi BleedingDocument3 pagesUpper Gi BleedingIkhwan HafrizNo ratings yet
- Burns & EscharotomyDocument36 pagesBurns & Escharotomyhatem alsrour100% (2)
- Necrotizing Soft Tissue InfectionsDocument15 pagesNecrotizing Soft Tissue InfectionsbengdubiNo ratings yet
- Spinal Cord Tumors: By: Divine Incillo Shiela Marie LaraDocument27 pagesSpinal Cord Tumors: By: Divine Incillo Shiela Marie LaraDivine IncilloNo ratings yet
- Necrotizing FasciitisDocument7 pagesNecrotizing FasciitisjoycefrancielleNo ratings yet
- Epidemiology of Oral Cancer PDFDocument6 pagesEpidemiology of Oral Cancer PDFمحمد عبدالهادي إسماعيلNo ratings yet
- Esophageal CancerDocument40 pagesEsophageal Cancerapi-282115150No ratings yet
- AppendicitisDocument29 pagesAppendicitisBintari AnindhitaNo ratings yet
- Thyroid Neoplasms: Kelompok 3 Dr. Reza Maulana Dr. Intan E. Napitupulu Drg. Andi Arfandi ArifuddinDocument41 pagesThyroid Neoplasms: Kelompok 3 Dr. Reza Maulana Dr. Intan E. Napitupulu Drg. Andi Arfandi ArifuddinIntan Eklesiana NapitupuluNo ratings yet
- Pancreatic CancerDocument25 pagesPancreatic CancerAatir JavaidNo ratings yet
- Burns: James Taclin C. Banez M.D., FPSGS, FPCSDocument48 pagesBurns: James Taclin C. Banez M.D., FPSGS, FPCSCodillia CheongNo ratings yet
- Principles of Cancer Treatment Col ShaziaDocument46 pagesPrinciples of Cancer Treatment Col ShaziaSammon TareenNo ratings yet
- Cervical CancerDocument36 pagesCervical CancerDebabrata SatapathyNo ratings yet
- Pancreatic MassDocument124 pagesPancreatic MassKMNo ratings yet
- Management of Thyroid DisordersDocument53 pagesManagement of Thyroid DisordersAnityo S AthmadjaNo ratings yet
- Surgical Infections Chapter 5 Shcwartz Principles of SurgeryDocument34 pagesSurgical Infections Chapter 5 Shcwartz Principles of Surgeryanas hindawi100% (4)
- Thyroid CancerDocument39 pagesThyroid CancerFaheem SarwarNo ratings yet
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- AnatomyDocument91 pagesAnatomysarahNo ratings yet
- Relining in RPD!Document33 pagesRelining in RPD!sarah50% (2)
- Introduction History Examination (Prosthodontics)Document37 pagesIntroduction History Examination (Prosthodontics)sarah0% (1)
- ENT Lecture!Document31 pagesENT Lecture!sarahNo ratings yet
- Odontomes and Odontogenic TumoursDocument16 pagesOdontomes and Odontogenic TumourssarahNo ratings yet
- Periodontology SeqDocument17 pagesPeriodontology SeqsarahNo ratings yet
- Oralmed SEQDocument8 pagesOralmed SEQsarahNo ratings yet
- Mj51 Project Management MiningDocument3 pagesMj51 Project Management MiningMarcial CastroNo ratings yet
- IBC PPT (Objectives and Grounds)Document3 pagesIBC PPT (Objectives and Grounds)Ameya Gawhane100% (1)
- After The Last Sheet.: Ronnie D. Caringal Canubing National High SchoolDocument15 pagesAfter The Last Sheet.: Ronnie D. Caringal Canubing National High SchoolThea Margareth MartinezNo ratings yet
- Unit 7Document4 pagesUnit 7Võ Việt NamNo ratings yet
- CET309Document12 pagesCET309dipinnediyaparambathNo ratings yet
- Security Rules in HRMS (Restrict Users)Document7 pagesSecurity Rules in HRMS (Restrict Users)zafariqbal_scribdNo ratings yet
- Acct Statement - XX6550 - 09122023Document6 pagesAcct Statement - XX6550 - 09122023seapause26No ratings yet
- InternshipDocument16 pagesInternshipVarsha Chaudhary100% (1)
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesRona Mei TiangcoNo ratings yet
- Chapter 18: Hierarchy of Intersection ControlDocument39 pagesChapter 18: Hierarchy of Intersection ControlAbdhul Khadhir ShalayarNo ratings yet
- ProjectDocument48 pagesProjectNarendra Chaudhari100% (1)
- 8.operators in JavaDocument29 pages8.operators in JavavamshiNo ratings yet
- Lebw4982 02Document52 pagesLebw4982 02alexanderponomarevNo ratings yet
- HRD-QOHSER-002 Application FormDocument7 pagesHRD-QOHSER-002 Application FormMajestik ggNo ratings yet
- Paradigma Penelitian Kualitatif From Creswell Book Ch.1&2Document5 pagesParadigma Penelitian Kualitatif From Creswell Book Ch.1&2Ferial FerniawanNo ratings yet
- BAKASHABA Charles TestimonialDocument2 pagesBAKASHABA Charles Testimonialbakashabacharles7No ratings yet
- Graham & Doddsville - Issue 39 - v13 - FINALDocument35 pagesGraham & Doddsville - Issue 39 - v13 - FINALMarco MessinaNo ratings yet
- Bird HDC High Density CleanerDocument2 pagesBird HDC High Density CleanerFaridUZamaNo ratings yet
- Summative Test in English 6Document3 pagesSummative Test in English 6joshNo ratings yet
- Mass Flow SiloDocument17 pagesMass Flow SiloBùi Hắc HảiNo ratings yet
- Setup and ConfigDocument2 pagesSetup and Configpradeep kumarNo ratings yet
- Professional Indemnity in ConstructionDocument35 pagesProfessional Indemnity in ConstructionMurat YilmazNo ratings yet
- Atos AramDocument6 pagesAtos AramBillouNo ratings yet
- Top 50 Things To Do in Abu DhabiDocument17 pagesTop 50 Things To Do in Abu DhabiCJ WalkerNo ratings yet
- AffaldPlus - Naestved - DenmarkDocument4 pagesAffaldPlus - Naestved - DenmarkJOHNKNo ratings yet
- Free and Forced ConvectionDocument7 pagesFree and Forced ConvectionBunty Perera83% (6)
- Experimental Research Karlang and Gabi As Paper BagDocument12 pagesExperimental Research Karlang and Gabi As Paper BagEdralyn LuadNo ratings yet
- CV FormatDocument3 pagesCV FormatSK ACADEMYNo ratings yet
- CSI Solution Demonstrates Use of These Features: Mesh Area Objects "Trick" ProblemDocument4 pagesCSI Solution Demonstrates Use of These Features: Mesh Area Objects "Trick" ProblemSofiane BensefiaNo ratings yet