You might also like
- Full Download Ebook Ebook PDF Microbiology Fundamentals A Clinical Approach 3rd Edition PDFDocument42 pagesFull Download Ebook Ebook PDF Microbiology Fundamentals A Clinical Approach 3rd Edition PDFmicheal.cooper974100% (1)
- Alternatives To VaccinationsDocument4 pagesAlternatives To VaccinationsNilanjan Ray100% (1)
- Osteoarthritis 191016103144Document49 pagesOsteoarthritis 191016103144dr.abouzaid098No ratings yet
- Wanita 18 Tahun Dengan Peritonitis TB Dan Tuberculosis Paru Kasus Baru Bta PositifDocument20 pagesWanita 18 Tahun Dengan Peritonitis TB Dan Tuberculosis Paru Kasus Baru Bta PositifNur IndayantiNo ratings yet
- Disseminated Intravacular Coagulation (DIC) 2Document12 pagesDisseminated Intravacular Coagulation (DIC) 2Radya AgnaNo ratings yet
- Makalah SleDocument48 pagesMakalah Slesalini_sadhna17No ratings yet
- English 10: Quarter 4 - Module 2 Giving Technical and Operational DefinitionsDocument21 pagesEnglish 10: Quarter 4 - Module 2 Giving Technical and Operational DefinitionsDdeow grtilNo ratings yet
- Patofisiologi & Penatalaksanaan Gagal Ginjal KronikDocument34 pagesPatofisiologi & Penatalaksanaan Gagal Ginjal KronikAvenaAthaliaNo ratings yet
- OMIC 311 Lecture 17 Human Papilloma, Herpes, Hepatits VirusDocument51 pagesOMIC 311 Lecture 17 Human Papilloma, Herpes, Hepatits VirusMaryam XANo ratings yet
- Enterobacteriaceae Handout (Lec & Lab)Document15 pagesEnterobacteriaceae Handout (Lec & Lab)Lucille MarieNo ratings yet
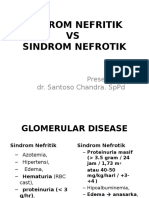
- Sindroma Nefrotik Vs NefritikDocument23 pagesSindroma Nefrotik Vs NefritikBetha456100% (1)
- Medical MCQ Center Tuberculosis MCQsDocument4 pagesMedical MCQ Center Tuberculosis MCQsBanu KubendiranNo ratings yet
- Hematologi Pada AnakDocument48 pagesHematologi Pada AnakRisma Orchita Agwisa FNo ratings yet
- Index Wayne N New Castle (Thyroid)Document1 pageIndex Wayne N New Castle (Thyroid)asyiqinramdan100% (1)
- Philippine Health Care Delivery System - FinalDocument62 pagesPhilippine Health Care Delivery System - FinalRyan Michael Oducado0% (1)
- SN Vs SNADocument26 pagesSN Vs SNAChofi QolbiNo ratings yet
- 03 - DR - Dominicus - PELATIHAN DIFTERI SMD 17 Jan 2018 - Diagnosis - SharedDocument54 pages03 - DR - Dominicus - PELATIHAN DIFTERI SMD 17 Jan 2018 - Diagnosis - SharedFebria Valentine AritonangNo ratings yet
- CholestasisDocument39 pagesCholestasisMukhtar JamacNo ratings yet
- Prof Linda Slide Thalasemia 2017Document44 pagesProf Linda Slide Thalasemia 2017IkaNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- Ectropion & EntropionDocument2 pagesEctropion & EntropionAhmed ShafikNo ratings yet
- OsteomielitisDocument28 pagesOsteomielitismaulidaangraini100% (1)
- Harrison Boli Infectioase 30pp7452Document30 pagesHarrison Boli Infectioase 30pp7452Камелия Калева100% (3)
- Kegawatan Bidang Penyakit Dalam GELSDocument55 pagesKegawatan Bidang Penyakit Dalam GELSwibowo0% (1)
- InsulinomaDocument16 pagesInsulinomaDerly Barino HasdiNo ratings yet
- Sindroma Nefrotik Vs NefritikDocument22 pagesSindroma Nefrotik Vs NefritikAyueka EkaNo ratings yet
- Sindroma Nefrotik Vs NefritikDocument23 pagesSindroma Nefrotik Vs NefritiksiayuNo ratings yet
- Nephritic Syndrome: Pyuza, MDDocument41 pagesNephritic Syndrome: Pyuza, MDawadh mbaroukNo ratings yet
- Sindrom NefrotikDocument13 pagesSindrom NefrotikWulan AzmiNo ratings yet
- GNA GNC PNC - PPSXDocument31 pagesGNA GNC PNC - PPSXMira AstutiNo ratings yet
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightNo ratings yet
- Gigantisme Dan AkromegaliDocument20 pagesGigantisme Dan AkromegaliNovia Sari Andriati MertosonoNo ratings yet
- Tatalaksana Lupus Nefritis, Dr. Edi HidayatDocument34 pagesTatalaksana Lupus Nefritis, Dr. Edi HidayatDr Edi Hidayat100% (1)
- Diagnosis & Tata Laksana Cad / CcsDocument40 pagesDiagnosis & Tata Laksana Cad / CcsIno HajrinNo ratings yet
- 2 DHF InternaDocument59 pages2 DHF Internasaladass 2No ratings yet
- Sindrom NefrotikDocument22 pagesSindrom NefrotikGyta Apriati100% (1)
- Empiema Kandung EmpeduDocument7 pagesEmpiema Kandung EmpeduHasya KinasihNo ratings yet
- Trombositosis Esensial: (Essential Thrombocytosis)Document9 pagesTrombositosis Esensial: (Essential Thrombocytosis)muslimNo ratings yet
- Pure Red Cell Aplasia PRCADocument14 pagesPure Red Cell Aplasia PRCANikkiRoxasNo ratings yet
- Acute Pulmonary Edema - NEJMDocument4 pagesAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- n378.008 Iris Website Staging of CKD PDFDocument8 pagesn378.008 Iris Website Staging of CKD PDFrutebeufNo ratings yet
- Pembahasan UKDI CLINIC 1 Batch Mei 2016Document535 pagesPembahasan UKDI CLINIC 1 Batch Mei 2016William Hartanto RusliNo ratings yet
- Format Penilaian Ketrampilan Pemeriksaan Fisik Head To ToeDocument18 pagesFormat Penilaian Ketrampilan Pemeriksaan Fisik Head To Toeayatun nadzirahNo ratings yet
- Leukimia Dan ThalasemiaDocument39 pagesLeukimia Dan ThalasemialeilaNo ratings yet
- Bunga Rampai Infeksi Dengue AnakDocument67 pagesBunga Rampai Infeksi Dengue AnakSatrio PrimaesoNo ratings yet
- HSP and ITPDocument2 pagesHSP and ITPSara Vowels-Hattaway100% (3)
- Congestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCDocument25 pagesCongestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCYUSRIL ZUMADINSYAHNo ratings yet
- Tonsillitis Diphteri: Literature ReadingDocument28 pagesTonsillitis Diphteri: Literature ReadingFebryantiPBundaayabariq100% (1)
- Djenkolism ToxificationDocument5 pagesDjenkolism ToxificationSilvia RizkaNo ratings yet
- Patofisiologi DysuriaDocument4 pagesPatofisiologi DysuriaCindy RolexzaNo ratings yet
- Disorders of PubertyDocument20 pagesDisorders of PubertyMuthia ArsilNo ratings yet
- Kolestasis Intrahepatal Vs EkstrahepatalDocument4 pagesKolestasis Intrahepatal Vs EkstrahepatalrikarikaNo ratings yet
- Diagnosa Banding Edema: Ginjal Dan Non GinjalDocument2 pagesDiagnosa Banding Edema: Ginjal Dan Non GinjalFezy Ezia Dwi Sister, S.Ked100% (1)
- Patogenesis SJS TENDocument2 pagesPatogenesis SJS TENpalmaria sitanggangNo ratings yet
- OsteoporosisDocument57 pagesOsteoporosisViviViviNo ratings yet
- Pure Red Cell AplasiaDocument3 pagesPure Red Cell AplasiaCitrusNo ratings yet
- Sindrom Hemolitik UremikDocument24 pagesSindrom Hemolitik UremikLindaaaNo ratings yet
- Komplikasi Dan Prognosis Demam TifoidDocument6 pagesKomplikasi Dan Prognosis Demam TifoidPundi Pandan Putri PinantiNo ratings yet
- Pemeriksaan Penunjang Creeping EruptionDocument6 pagesPemeriksaan Penunjang Creeping EruptionMaulia RahmaNo ratings yet
- Sindrom NefrotikDocument31 pagesSindrom NefrotikMohammed Ramzy GhifariNo ratings yet
- Penatalaksanaan IRISDocument39 pagesPenatalaksanaan IRISdian sudianaNo ratings yet
- Sindroma Nefrotik Vs NefritikDocument23 pagesSindroma Nefrotik Vs NefritikUswatun Aortatika KhasanahNo ratings yet
- Sindroma Nefrotik Vs NefritikDocument23 pagesSindroma Nefrotik Vs NefritikihsanNo ratings yet
- Sindrom Nefritik DebDocument2 pagesSindrom Nefritik DebrchristevenNo ratings yet
- Glomerular Disease: Naifah Luthfiyah Putri 1510211009Document41 pagesGlomerular Disease: Naifah Luthfiyah Putri 1510211009NaifahLuthfiyahPutriNo ratings yet
- Pathology of Common Glomerular Syndromes: DR Purushotham KrishnappaDocument34 pagesPathology of Common Glomerular Syndromes: DR Purushotham KrishnappaTarin IslamNo ratings yet
- Approach Nefroritic SXDocument58 pagesApproach Nefroritic SX[ qιlα ]No ratings yet
- Glomerulonephritis 2Document56 pagesGlomerulonephritis 2Mans FansNo ratings yet
- Nephrotic Syndrome in ChildrenDocument33 pagesNephrotic Syndrome in ChildrenAlvin Omondi100% (1)
- UV PlusDocument3 pagesUV PlusCrysuci MeiliningtyasNo ratings yet
- Viruses As Biological Control AgentsDocument17 pagesViruses As Biological Control AgentsJohn BildanNo ratings yet
- 1.conjunctiva and ConjunctivitisDocument77 pages1.conjunctiva and ConjunctivitisPreeti PatelNo ratings yet
- Agar Gel Precipitation...Document47 pagesAgar Gel Precipitation...fedhawakNo ratings yet
- Tabla Patologia PDFDocument151 pagesTabla Patologia PDFJuan Carlos HernandezNo ratings yet
- 10 Bahasa Indonesia Kasus Kehamilan MelahirkanDocument164 pages10 Bahasa Indonesia Kasus Kehamilan Melahirkancuuphy meryliantNo ratings yet
- MAPEH 8 Quarter 3 WEEK 5-6 (MODULE) MusicDocument4 pagesMAPEH 8 Quarter 3 WEEK 5-6 (MODULE) MusicMirela CalubayanNo ratings yet
- CHN Practice Questions PDFDocument19 pagesCHN Practice Questions PDFMichaela D. Velasco100% (1)
- Seroprevallance of Brucellosis MalitensisDocument50 pagesSeroprevallance of Brucellosis MalitensisAbdiNo ratings yet
- Food Safety and SecurityDocument14 pagesFood Safety and SecurityKate ManalansangNo ratings yet
- Bio 213 Gram Positive and NegativeDocument4 pagesBio 213 Gram Positive and NegativeMaclord GolvinNo ratings yet
- HPV Vaccine and Males Issues and ChallengesDocument6 pagesHPV Vaccine and Males Issues and ChallengesBonnie WangNo ratings yet
- Unit 4Document2 pagesUnit 4Bea Bolaños MenaNo ratings yet
- Caregiving Lesson Quarter ExamsDocument3 pagesCaregiving Lesson Quarter ExamsGlaiza FloresNo ratings yet
- UNIT 8 Special Issues in The Delivery of Transculture Nursing CareDocument8 pagesUNIT 8 Special Issues in The Delivery of Transculture Nursing CareMushtaq Ali100% (2)
- DiseaseDocument6 pagesDiseasekomal Raj ShresthaNo ratings yet
- Jafar Mohd'Document39 pagesJafar Mohd'LeenCo TechNo ratings yet
- FilarianDocument9 pagesFilarianEricsson CarabbacanNo ratings yet
- Q3 G9 English M2Document32 pagesQ3 G9 English M2Maria Camel PeñarandaNo ratings yet
- Ujjol MainDocument6 pagesUjjol MaintashfimmironNo ratings yet
- Salmonella PPT PresentationDocument29 pagesSalmonella PPT PresentationAbcdefg HijklNo ratings yet