You might also like
- Chapter 067 Sirs ModsDocument25 pagesChapter 067 Sirs Modsapi-232466940No ratings yet
- SketchyPath ChecklistDocument1 pageSketchyPath ChecklistFajar Raza100% (1)
- Cardiogenic Shock PDFDocument14 pagesCardiogenic Shock PDFAdreiTheTripleANo ratings yet
- SepsisDocument33 pagesSepsisv_vijayakanth7656No ratings yet
- Neuroanatomy Draw It To Know ItDocument477 pagesNeuroanatomy Draw It To Know ItLiangrid Nunes Barroso RodriguesNo ratings yet
- Intestinal Obstruction: EpidemiologyDocument11 pagesIntestinal Obstruction: EpidemiologyBereket temesgenNo ratings yet
- Neurogenic Shock (New)Document14 pagesNeurogenic Shock (New)Syarafina AminuddinNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Nursing Care of Clients With Cardiovascular DisorderDocument16 pagesNursing Care of Clients With Cardiovascular DisorderLuna MarieNo ratings yet
- Cardiac TamponadeDocument10 pagesCardiac TamponadeRahmi Fatma SariNo ratings yet
- Reproductive Endocrinology For Gynaecologist SDocument356 pagesReproductive Endocrinology For Gynaecologist SFebey Arie Mulya100% (1)
- Hepatic Encephalopathy and ComaDocument19 pagesHepatic Encephalopathy and ComaJas Castro JoveroNo ratings yet
- Class Presentation ON Acute Tubular NecrosisDocument39 pagesClass Presentation ON Acute Tubular NecrosisDeeksha RajputNo ratings yet
- The Normal and Pathological Fetal Brain - Ultrasonographic FeaturesDocument316 pagesThe Normal and Pathological Fetal Brain - Ultrasonographic FeaturesBharti Pant GahtoriNo ratings yet
- Word Part: Word Part Meaning Example(s) Meaning of Example(s)Document6 pagesWord Part: Word Part Meaning Example(s) Meaning of Example(s)Anonymous zdHKF34HNo ratings yet
- Integumentary System ReviewerDocument6 pagesIntegumentary System ReviewerKrize Colene dela CruzNo ratings yet
- 978 0323049092 Color Textbook of Pediatric Dermatology Color Textbook of Pediatric Dermatology WestonDocument61 pages978 0323049092 Color Textbook of Pediatric Dermatology Color Textbook of Pediatric Dermatology Westonaudrey.walston606100% (42)
- Cardiac Enzyme StudiesDocument4 pagesCardiac Enzyme StudiesDara VinsonNo ratings yet
- Pharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Document23 pagesPharmacology Assignment No.02: Submitted By: Submitted To: Nandraj Ma'am Areeba Shafiq Roll No. 1817007Nandraj123100% (1)
- Myocardialinfarction 150223043527 Conversion Gate02 PDFDocument22 pagesMyocardialinfarction 150223043527 Conversion Gate02 PDFBhavika Aggarwal100% (1)
- Cardiogenic ShockDocument20 pagesCardiogenic Shockanimesh pandaNo ratings yet
- Hyponatremia: Presenter: DR Arun Karmakar Moderator: Prof. N. SharatkumarDocument50 pagesHyponatremia: Presenter: DR Arun Karmakar Moderator: Prof. N. SharatkumarLyra FebriandaNo ratings yet
- Massive BleedingpptDocument24 pagesMassive BleedingpptFidel Gimotea Yongque IIINo ratings yet
- What Are Electrolytes? What Causes Electrolyte Imbalance?: Fast Facts On ElectrolytesDocument11 pagesWhat Are Electrolytes? What Causes Electrolyte Imbalance?: Fast Facts On ElectrolytesL InfiniteNo ratings yet
- EUROIMMUNDocument66 pagesEUROIMMUNOskar Z ChávezNo ratings yet
- Myasthenia GravisDocument45 pagesMyasthenia GravisVirgilio Reyes ManuelNo ratings yet
- HypertensionDocument20 pagesHypertensiondocbayNo ratings yet
- Renal Calculi IntroductionDocument4 pagesRenal Calculi IntroductionirysatherfinestNo ratings yet
- Large Intestine HistologyDocument24 pagesLarge Intestine HistologyMudassar RoomiNo ratings yet
- Pulmonaryembolism 150329161109 Conversion Gate01Document60 pagesPulmonaryembolism 150329161109 Conversion Gate01Rafika RaraNo ratings yet
- Shock and SIRSDocument85 pagesShock and SIRSBryan Mae H. DegorioNo ratings yet
- Tissue TransplantDocument20 pagesTissue TransplantEva Boje-JugadorNo ratings yet
- Concept Map AAADocument6 pagesConcept Map AAASandrine BarredoNo ratings yet
- Cholesistitis (DR - Prema Hapsari, SPPD)Document28 pagesCholesistitis (DR - Prema Hapsari, SPPD)Niniek Iin F100% (1)
- NocturiaDocument10 pagesNocturiaKousik AmancharlaNo ratings yet
- Understanding Traumatic Brain InjuryDocument43 pagesUnderstanding Traumatic Brain InjurySilvanaPutriNo ratings yet
- LeukemiaDocument23 pagesLeukemiaSrm GeneticsNo ratings yet
- N24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis AsthmaDocument42 pagesN24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis Asthmadentist40No ratings yet
- Pathophysiology of Head TraumaDocument12 pagesPathophysiology of Head TraumaMohammad ZianuddinNo ratings yet
- Valvularheart Diseases: PathophysiologyDocument9 pagesValvularheart Diseases: PathophysiologyVoid LessNo ratings yet
- Antineoplastic DrugsDocument16 pagesAntineoplastic DrugstheintrovNo ratings yet
- Pathophysiology of InfectionDocument3 pagesPathophysiology of Infectionchristianemmanuel18No ratings yet
- Pathophysiology 2Document92 pagesPathophysiology 2Princess AgarwalNo ratings yet
- Cad ....Document94 pagesCad ....AnanthibalaNo ratings yet
- Prepared By: Germany de GuzmanDocument13 pagesPrepared By: Germany de GuzmanBeauMee Maglasang Bustillo-LlanoNo ratings yet
- Emphysematous Pyelonephritis (EPN)Document31 pagesEmphysematous Pyelonephritis (EPN)HardiTariqHammaNo ratings yet
- An Overview Of: Acute Kidney Injury (Aki: Hasan BasriDocument22 pagesAn Overview Of: Acute Kidney Injury (Aki: Hasan BasriDz PutraNo ratings yet
- Anterior Cord SyndromeDocument8 pagesAnterior Cord SyndromeJanine Erika Julom BrillantesNo ratings yet
- Myasthenia Gravis: An Autoimmune Neurologic DisorderDocument16 pagesMyasthenia Gravis: An Autoimmune Neurologic DisorderHibba NasserNo ratings yet
- CarboplatinDocument10 pagesCarboplatinapi-273179395No ratings yet
- Disorders of The EyeDocument16 pagesDisorders of The Eyelisette_sakuraNo ratings yet
- Myocardial InfarctionDocument15 pagesMyocardial InfarctionameerNo ratings yet
- CardioDocument7 pagesCardioGerald AndrinNo ratings yet
- Chronic Renal FailureDocument26 pagesChronic Renal FailurePriya GandhiNo ratings yet
- A Case Report of Classical Hodgkin's Lymphoma Presented With Anemia of Chronic Disease As Microcytic Hypochromic TypeDocument3 pagesA Case Report of Classical Hodgkin's Lymphoma Presented With Anemia of Chronic Disease As Microcytic Hypochromic TypeIOSRjournalNo ratings yet
- Head Injury: Manali H. Solanki F.Y. M.Sc. Nursing J G College of NursingDocument31 pagesHead Injury: Manali H. Solanki F.Y. M.Sc. Nursing J G College of NursingWaqar AhmedNo ratings yet
- What Is Hypertensive NephropathyDocument11 pagesWhat Is Hypertensive NephropathyIvy Pamanian DeldaNo ratings yet
- CT KubDocument2 pagesCT KubKumail KhandwalaNo ratings yet
- Edema: Dr. Bernardo Dámaso MataDocument55 pagesEdema: Dr. Bernardo Dámaso MataDeivis Dan ErickNo ratings yet
- StrokeDocument12 pagesStrokeSam JamesNo ratings yet
- Acoustic NeuromaDocument23 pagesAcoustic Neuromacefiroth100% (1)
- Heart Failure With Preserved Ejection FractionDocument19 pagesHeart Failure With Preserved Ejection Fractioncosmin balanNo ratings yet
- AnginaDocument17 pagesAnginaGaming ModeNo ratings yet
- PyelonephritisDocument10 pagesPyelonephritisalina abu rumi100% (1)
- Adrenergic AgonistsDocument18 pagesAdrenergic AgonistsJod Bell100% (1)
- NCM100 Cystoclysis CareDocument2 pagesNCM100 Cystoclysis CarecchiechieNo ratings yet
- Hepatobiliary Disorders 2Document21 pagesHepatobiliary Disorders 2KatrinaJimenezNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Function of Platelets 1Document13 pagesFunction of Platelets 1deput_rprNo ratings yet
- SupsDocument3 pagesSupsasdfasdfawefawefNo ratings yet
- Grade 3 Cot Filipino Pandiwa q4Document9 pagesGrade 3 Cot Filipino Pandiwa q4Maricar FaralaNo ratings yet
- Life Sciences Answers For Remote Learning Workbook Term 3Document24 pagesLife Sciences Answers For Remote Learning Workbook Term 3Anathiey Certified Jnr.No ratings yet
- Contorno de Órgão de Risco Thoracic Radiation TherapyDocument106 pagesContorno de Órgão de Risco Thoracic Radiation TherapyLEONARDO CORDEIRO PEREIRANo ratings yet
- B5 Home AssignmentDocument2 pagesB5 Home AssignmentMemoona GullNo ratings yet
- Torso GuideDocument373 pagesTorso GuideMonica PatracutaNo ratings yet
- Polycystic Kidney DiseaseDocument6 pagesPolycystic Kidney DiseaseRimsha Khan100% (1)
- Physiology Questions and Outlines: Sen. Odokoro Obumneme Michael (Power Mike)Document35 pagesPhysiology Questions and Outlines: Sen. Odokoro Obumneme Michael (Power Mike)Chinweuba ChristopherNo ratings yet
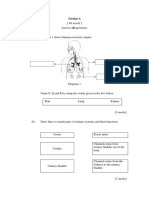
- Section A: Jawab Semua SoalanDocument3 pagesSection A: Jawab Semua SoalanAzreen IzetNo ratings yet
- L 10 Reaching The Age of Adolescence Exercise QuestionsDocument7 pagesL 10 Reaching The Age of Adolescence Exercise QuestionssantoshNo ratings yet
- Exam 2 ReviewDocument31 pagesExam 2 ReviewAhsan Tebha50% (2)
- Hypertensive Emergency and UrgencyDocument12 pagesHypertensive Emergency and UrgencyharshiniNo ratings yet
- Science G4 Break It DownDocument51 pagesScience G4 Break It DownYourMakatiPad Properties100% (1)
- Nodular Goiter Concept MapDocument5 pagesNodular Goiter Concept MapAllene PaderangaNo ratings yet
- 2010 NRN2833 Keysers Kaas GazzolaDocument12 pages2010 NRN2833 Keysers Kaas GazzolaRenzo LanfrancoNo ratings yet
- Grade 6 - SSES - Science - Q2 - Wk1 - GLAKDocument16 pagesGrade 6 - SSES - Science - Q2 - Wk1 - GLAKMelanie TrinidadNo ratings yet
- Hes006 CNS Lab 15 18Document50 pagesHes006 CNS Lab 15 18Joana Elizabeth A. CastroNo ratings yet
- NUR11O1 Integrated Human Anatomy and Physiology Department of Biology Institute of Arts and Sciences Far Eastern UniversityDocument5 pagesNUR11O1 Integrated Human Anatomy and Physiology Department of Biology Institute of Arts and Sciences Far Eastern UniversityPrancheska Abigayle Peneyra SantiagoNo ratings yet
- The Nervous System: by - Brett Bennell and Lisa MatzelleDocument27 pagesThe Nervous System: by - Brett Bennell and Lisa MatzelleJames PerianayagamNo ratings yet
- Unit 5 - Kidney and NephronDocument30 pagesUnit 5 - Kidney and NephronAbdullah MohammedNo ratings yet