You might also like
- The Management of Pressure Ulcers in Primary and Secondary Care PDFDocument464 pagesThe Management of Pressure Ulcers in Primary and Secondary Care PDFDragos-Ronald RugescuNo ratings yet
- Basic InstrumentationDocument55 pagesBasic Instrumentationmirai desu100% (1)
- Surgical InstrumentDocument59 pagesSurgical InstrumentCHALIE MEQUNo ratings yet
- Operating Room InstrumentsDocument59 pagesOperating Room InstrumentsMayolianne Dumay100% (1)
- Surgical Draping: Dr. Aidah Abu Elsoud Alkaissi An Najah National University Faculty of NursingDocument17 pagesSurgical Draping: Dr. Aidah Abu Elsoud Alkaissi An Najah National University Faculty of NursingBrigette Jane Michelle MartilNo ratings yet
- WK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TideDocument43 pagesWK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TidePotato PceeNo ratings yet
- IV TherapyDocument39 pagesIV TherapyChannelGNo ratings yet
- CPR Checklist PDFDocument2 pagesCPR Checklist PDFSakura SaitoNo ratings yet
- Foreigh Body Airway Obstruction Management July 2019Document1 pageForeigh Body Airway Obstruction Management July 2019Feliros S. SanciangcoNo ratings yet
- Preoperative PreparationDocument22 pagesPreoperative Preparationjackyploes100% (1)
- Medical Surgical NursingDocument237 pagesMedical Surgical NursingabdulhafezjamasariNo ratings yet
- Oncology Lectures 1 7 DR - FerrolinoDocument24 pagesOncology Lectures 1 7 DR - FerrolinoMiguel Cuevas DolotNo ratings yet
- Initial Assessment AND ManagementDocument30 pagesInitial Assessment AND ManagementSikaNo ratings yet
- Trauma and Emergency NursingDocument9 pagesTrauma and Emergency Nursingchinthaka18389021No ratings yet
- Intracranial Hypertension or Increased ICPDocument11 pagesIntracranial Hypertension or Increased ICPRomina Irish MatutinoNo ratings yet
- W1L1 - Initial Assessment For Trauma - 2Document44 pagesW1L1 - Initial Assessment For Trauma - 2Baihaqi SaharunNo ratings yet
- The Resister, The Political Warfare Journal of The Special Forces UndergroundVolume I, Number 3 Winter 1994Document28 pagesThe Resister, The Political Warfare Journal of The Special Forces UndergroundVolume I, Number 3 Winter 1994Rmplstlskn100% (1)
- Or ConceptsDocument70 pagesOr ConceptsArnulfo ArmamentoNo ratings yet
- Rabies: Rabies Is A Zoonotic Disease (A Disease That Is Transmitted To Humans From Animals) That Is Caused by A VirusDocument21 pagesRabies: Rabies Is A Zoonotic Disease (A Disease That Is Transmitted To Humans From Animals) That Is Caused by A VirusSabita Gangadeen100% (1)
- AcromegalyDocument24 pagesAcromegalycsngiuNo ratings yet
- BSN3-1 Perioperative-Nursing 2021Document236 pagesBSN3-1 Perioperative-Nursing 2021Ms MedSurg Nursin100% (2)
- Tubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterDocument11 pagesTubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterJeremy HamptonNo ratings yet
- Wound Documentation Tips PDFDocument2 pagesWound Documentation Tips PDFWinnie LiNo ratings yet
- CPG Unstable AnginaDocument58 pagesCPG Unstable AnginaAmir HassenNo ratings yet
- OR InstrumentsDocument56 pagesOR Instrumentssellyna SaidinNo ratings yet
- Health Questionnaire CandidateDocument5 pagesHealth Questionnaire CandidateSaudia Arabia JobsNo ratings yet
- Triage Lecture DR F Mesa GaerlanDocument55 pagesTriage Lecture DR F Mesa Gaerlanapi-19431894100% (1)
- Management of Multiple Traumatised PatientDocument4 pagesManagement of Multiple Traumatised PatientOmar MohammedNo ratings yet
- The Operating TheatreDocument30 pagesThe Operating TheatrePrincewill SeiyefaNo ratings yet
- Cell Ab Midterm MesiDocument7 pagesCell Ab Midterm MesiSamantha VeraNo ratings yet
- Report in Respiratory SuctioningDocument29 pagesReport in Respiratory SuctioningWendy EscalanteNo ratings yet
- итоговое заданиеDocument2 pagesитоговое заданиеOlga Kukhtina100% (1)
- Basic Surgical Instruments: by DR H - El SharkawyDocument60 pagesBasic Surgical Instruments: by DR H - El SharkawyNia Kurnia100% (1)
- History of The Suture Personal Suture Preference Suture CharacteristicsDocument33 pagesHistory of The Suture Personal Suture Preference Suture Characteristicsmob3No ratings yet
- Summative Exam 4 Sets Inquiry, Investigation and ImmersionDocument7 pagesSummative Exam 4 Sets Inquiry, Investigation and ImmersionAruel Delim100% (4)
- Initial Assessment of The Trauma PatientDocument36 pagesInitial Assessment of The Trauma PatientDr.G.Bhanu PrakashNo ratings yet
- Emergency and Disaster NursingDocument101 pagesEmergency and Disaster NursingJnll SbNo ratings yet
- Perioperative Nursing - 2edited For BSN 3Document122 pagesPerioperative Nursing - 2edited For BSN 3JL D. BusiaNo ratings yet
- Fishing in The Roman WorldDocument69 pagesFishing in The Roman Worldmnm06100% (1)
- Baseline Vital Kefah 1ADocument38 pagesBaseline Vital Kefah 1AShahd Abu SnenehNo ratings yet
- Dounis Interview PDFDocument15 pagesDounis Interview PDFNilson Marcos SoaresNo ratings yet
- Multiple Choice Spelling and Greeting SammyDocument6 pagesMultiple Choice Spelling and Greeting SammymallaNo ratings yet
- MEDDEV 2 - 7 - 1 - Rev4 - enDocument65 pagesMEDDEV 2 - 7 - 1 - Rev4 - enSalvatore CannataNo ratings yet
- Abdominalparacentesis 131005010712 Phpapp02Document33 pagesAbdominalparacentesis 131005010712 Phpapp02Shrish Pratap SinghNo ratings yet
- Nsg241 Study Guide Exam 5Document76 pagesNsg241 Study Guide Exam 5NatalieAndersonNo ratings yet
- Myasthenia GravisDocument24 pagesMyasthenia GravisAliMalikNo ratings yet
- Vera Pawlowsky-Glahn - Compositional Data Analysis in The Geosciences - From Theory To Practice-Geological Society (2006)Document214 pagesVera Pawlowsky-Glahn - Compositional Data Analysis in The Geosciences - From Theory To Practice-Geological Society (2006)javicol70No ratings yet
- 3119 01 6RP AFP tcm142-665726Document14 pages3119 01 6RP AFP tcm142-665726gulshanNo ratings yet
- Surgical Instruments RevisedDocument62 pagesSurgical Instruments RevisedDennis James BartolomeNo ratings yet
- S09-3 Compressor CTN10-16 (1.00)Document34 pagesS09-3 Compressor CTN10-16 (1.00)Anonymous AW4pRV7r75% (4)
- Infectious Disease Awareness In, Mogadishu, SomaliaDocument7 pagesInfectious Disease Awareness In, Mogadishu, Somaliashafie Mohamed AliNo ratings yet
- Pulmonary EmbolismDocument19 pagesPulmonary EmbolismIbrahimNo ratings yet
- 14 - PoleñoDocument9 pages14 - PoleñoPebbles PangilinanNo ratings yet
- Ivt Procedure With RationaleDocument10 pagesIvt Procedure With RationalelilileeNo ratings yet
- OncologyDocument5 pagesOncologymitzi019No ratings yet
- Bacterial Infections of The Skin, Soft TissuesDocument27 pagesBacterial Infections of The Skin, Soft TissuesSHIHAB UDDIN KAZI100% (1)
- Or NursingDocument48 pagesOr NursingJenn Botal Baguidudol100% (1)
- Cte #2: Matrix of Communicable DiseasesDocument7 pagesCte #2: Matrix of Communicable Diseasesjoannamae molagaNo ratings yet
- NANDA DX NI, NODocument165 pagesNANDA DX NI, NOKerry Brown100% (1)
- Perioperative Education Perioperative Team Sir MarkDocument31 pagesPerioperative Education Perioperative Team Sir Markfiel borataNo ratings yet
- Esi (1Document114 pagesEsi (1Ferina Mega SilviaNo ratings yet
- Suturing!: Prologue Course Directors Ucsf Department of Surgery Harras Zaid and Derek Ward, MsiisDocument20 pagesSuturing!: Prologue Course Directors Ucsf Department of Surgery Harras Zaid and Derek Ward, MsiisHarkanNo ratings yet
- Prehospital Hemorrhage Control and Treatment by Clinicians A Joint Position StatementDocument15 pagesPrehospital Hemorrhage Control and Treatment by Clinicians A Joint Position StatementPaulMoreanoNo ratings yet
- 3) Buku Log Clinical Practice Record PERIOPERATIVE CAREDocument41 pages3) Buku Log Clinical Practice Record PERIOPERATIVE CAREAslam AssandakaniNo ratings yet
- CANCER History of Cancer Chemotherapy 2008Document12 pagesCANCER History of Cancer Chemotherapy 2008gustavopsoNo ratings yet
- 2008 Classification and Management of Acute WoundsDocument5 pages2008 Classification and Management of Acute WoundsMiguel Angel Carrasco MedinaNo ratings yet
- NPWT Renasys and Pico Clinical GuidelinesDocument78 pagesNPWT Renasys and Pico Clinical GuidelinesArdianto SucintaNo ratings yet
- Securing and Suctioning Endotracheal TubeDocument28 pagesSecuring and Suctioning Endotracheal TubeJohn Mark ParacadNo ratings yet
- 预备微积分2024参考试卷#2 学生Document51 pages预备微积分2024参考试卷#2 学生hqy1993goodNo ratings yet
- ABB Controls Training Brochure Jul-Dec 2014 PDFDocument4 pagesABB Controls Training Brochure Jul-Dec 2014 PDFpurwantoNo ratings yet
- Formula Games ModuleDocument27 pagesFormula Games ModuleJoy VidalNo ratings yet
- Gas Filter SizingDocument148 pagesGas Filter SizingRAJIV_332693187No ratings yet
- EVANGELISM Church PlantingDocument9 pagesEVANGELISM Church PlantingLeon LwambaNo ratings yet
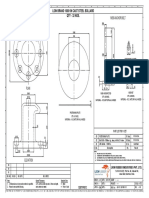
- M56 Anchor Bolt: Lion Brand 1000 KN Cast Steel Bollard Qty - 32 NosDocument1 pageM56 Anchor Bolt: Lion Brand 1000 KN Cast Steel Bollard Qty - 32 NossanaNo ratings yet
- Grades 9,10 Revision SheetsDocument22 pagesGrades 9,10 Revision SheetsALKHANSAA ELOBEIDYNo ratings yet
- LUNA V60 Recipe For 25g. Pourover To ShareDocument1 pageLUNA V60 Recipe For 25g. Pourover To ShareStevi FebriantoNo ratings yet
- Implementing Sales 12Document566 pagesImplementing Sales 12Amer YehiaNo ratings yet
- E646Document12 pagesE646Hillary McgowanNo ratings yet
- 0580 Y12 Ecr P2 v2Document45 pages0580 Y12 Ecr P2 v2Kay SinghNo ratings yet
- CXS 192eDocument396 pagesCXS 192eSubs KatsNo ratings yet
- 810900C Operating and Service Manual CIM 6 - 2009Document220 pages810900C Operating and Service Manual CIM 6 - 2009carlos santovalNo ratings yet
- What Is ReactDocument40 pagesWhat Is Reacthabtamu fentewNo ratings yet
- Module 1 2nd Quarter d11Document5 pagesModule 1 2nd Quarter d11Abbie RañosaNo ratings yet
- Dr. B. R. Ambedkar School of Specialized Excellence Sec 11, Rohini - 20231209 - 210444 - 0000Document2 pagesDr. B. R. Ambedkar School of Specialized Excellence Sec 11, Rohini - 20231209 - 210444 - 0000shivam2009sharma14No ratings yet
- SMS2008 DX33Document4 pagesSMS2008 DX33Imam DinNo ratings yet
- PR ExamDocument6 pagesPR Exambernmarr100% (1)
- Resultant of Concurrent Force System - Engineering Mechanics ReviewDocument2 pagesResultant of Concurrent Force System - Engineering Mechanics Reviewimrancenakk0% (2)
- 3483-Article Text-8498-2-10-20201015Document15 pages3483-Article Text-8498-2-10-20201015Nawzi kagimboNo ratings yet