You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Morning Report Case: Februari 19, 2010Document17 pagesMorning Report Case: Februari 19, 2010Felicia adeline ChristianNo ratings yet
- Bee Sting Case ReportDocument22 pagesBee Sting Case ReportFelicia adeline ChristianNo ratings yet
- COPD + Acute ExacerbationDocument23 pagesCOPD + Acute ExacerbationFelicia adeline ChristianNo ratings yet
- MR AnafilaksisDocument23 pagesMR AnafilaksisFelicia adeline ChristianNo ratings yet
- Morning Report: Friday 20 April 2012Document18 pagesMorning Report: Friday 20 April 2012Felicia adeline ChristianNo ratings yet
- MR SipDocument26 pagesMR SipFelicia adeline ChristianNo ratings yet
- Morning Report Case: June 18th, 2012Document13 pagesMorning Report Case: June 18th, 2012Felicia adeline ChristianNo ratings yet
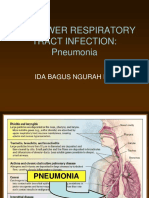
- The Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiDocument32 pagesThe Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiFelicia adeline ChristianNo ratings yet
- MR AnafilaksisDocument23 pagesMR AnafilaksisFelicia adeline ChristianNo ratings yet
- Morning Report Case: 18th July, 2012Document19 pagesMorning Report Case: 18th July, 2012Felicia adeline ChristianNo ratings yet
- MR IleusDocument24 pagesMR IleusFelicia adeline ChristianNo ratings yet
- The Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiDocument32 pagesThe Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiFelicia adeline ChristianNo ratings yet
- Morning Report Case: 16th July, 2012Document18 pagesMorning Report Case: 16th July, 2012Felicia adeline ChristianNo ratings yet
- Morning Report Case: 16th July, 2012Document20 pagesMorning Report Case: 16th July, 2012Felicia adeline ChristianNo ratings yet
- Morning Report Case: 7th October, 2011Document29 pagesMorning Report Case: 7th October, 2011Felicia adeline ChristianNo ratings yet
- Morning Report Case: October 27 2010Document33 pagesMorning Report Case: October 27 2010Felicia adeline ChristianNo ratings yet
- Morning Report Case: Februari 19, 2010Document17 pagesMorning Report Case: Februari 19, 2010Felicia adeline ChristianNo ratings yet
- Textbook ReadingDocument42 pagesTextbook ReadingFelicia adeline ChristianNo ratings yet
- LeptospirosisDocument19 pagesLeptospirosisFelicia adeline ChristianNo ratings yet
- Morning Report Case: June 18th, 2012Document13 pagesMorning Report Case: June 18th, 2012Felicia adeline ChristianNo ratings yet
- Journal ReadingDocument13 pagesJournal ReadingFelicia adeline ChristianNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Service Manual: Mds-Ja20EsDocument84 pagesService Manual: Mds-Ja20Esfoxmulder6161695No ratings yet
- Oil & Gas Amine Sweetening Unit ManualDocument56 pagesOil & Gas Amine Sweetening Unit ManualAariz Khan100% (2)
- Solutions of Mini Case Bruce HoniballDocument5 pagesSolutions of Mini Case Bruce HoniballShivshankar Yadav100% (1)
- Mushroom Umami Taste EvaluationDocument10 pagesMushroom Umami Taste EvaluationMaryam HanifNo ratings yet
- Carte Blanche: The New James Bond Novel by Jeffery DeaverDocument12 pagesCarte Blanche: The New James Bond Novel by Jeffery DeaverSimon and Schuster0% (1)
- Nominal Pipe Size, Nominal Diameter & Outside Diameter For PipesDocument1 pageNominal Pipe Size, Nominal Diameter & Outside Diameter For PipesmdnorNo ratings yet
- Script For TourguidingDocument2 pagesScript For Tourguidingfshe2677% (125)
- On K-Distance Degree Index of TreesDocument5 pagesOn K-Distance Degree Index of TreesVelumani sNo ratings yet
- Intel Processors PDFDocument33 pagesIntel Processors PDFbiplab royNo ratings yet
- Hematological Conditions QUESTIONSDocument9 pagesHematological Conditions QUESTIONSCJ RelleveNo ratings yet
- BA Anchor Data SheetDocument17 pagesBA Anchor Data SheetbrodieNo ratings yet
- Process Modeling in The Pharmaceutical Industry Using The Discrete Element MethodDocument29 pagesProcess Modeling in The Pharmaceutical Industry Using The Discrete Element MethodRonaldo MenezesNo ratings yet
- Zaldivar Et Al. 2017 (Dopamine Is Signaled by Mid-Frequency Oscillations and Boosts Output Layers Visual Information in Visual Cortex)Document30 pagesZaldivar Et Al. 2017 (Dopamine Is Signaled by Mid-Frequency Oscillations and Boosts Output Layers Visual Information in Visual Cortex)FRANCISCO ELI LEZAMA GUTIERREZNo ratings yet
- MTD Big Bore Engines 78 277cc 83 357cc 90 420cc Repair Manual PDFDocument136 pagesMTD Big Bore Engines 78 277cc 83 357cc 90 420cc Repair Manual PDFGiedrius MalinauskasNo ratings yet
- Algebra II PreAP SimplificationDocument4 pagesAlgebra II PreAP SimplificationSummer SharmaNo ratings yet
- Wall Mounted Wireless Air ConditionersDocument2 pagesWall Mounted Wireless Air ConditionerspenavicbNo ratings yet
- Introduction To Coal Handling PlantDocument12 pagesIntroduction To Coal Handling PlantPramod R BidveNo ratings yet
- MiG 21Document29 pagesMiG 21Zoran Vulovic100% (2)
- The Efficient Way To Prevent Water Carryover and Keep Your Indoor Air HealthierDocument1 pageThe Efficient Way To Prevent Water Carryover and Keep Your Indoor Air HealthierAzrinshah Abu BakarNo ratings yet
- Hurqalya - HavarqalyaDocument64 pagesHurqalya - HavarqalyaBVILLARNo ratings yet
- 241-Article Text-1014-1-10-20201017Document8 pages241-Article Text-1014-1-10-20201017derismurib4No ratings yet
- Agribusiness ManagementDocument20 pagesAgribusiness Managementronald_leabresNo ratings yet
- DTP - Digital Transformer ProtectionDocument13 pagesDTP - Digital Transformer ProtectionHBNBILNo ratings yet
- White Chicken KormaDocument5 pagesWhite Chicken Kormamkm2rajaNo ratings yet
- NIA045462022 KL 13 AR 1130 Royal Enfield Motors LTD Classic X 350 ESDocument10 pagesNIA045462022 KL 13 AR 1130 Royal Enfield Motors LTD Classic X 350 ESAkhil DasNo ratings yet
- 5 Commandments of DatingDocument8 pages5 Commandments of DatingBariki MwasagaNo ratings yet
- Atoms & Ions Worksheet 1 /63: Atomic Number and Mass NumberDocument4 pagesAtoms & Ions Worksheet 1 /63: Atomic Number and Mass Numbercate christineNo ratings yet
- Hazardous Waste Identification GuidanceDocument105 pagesHazardous Waste Identification GuidanceMiguel TorresNo ratings yet
- Pol Science ProjectDocument18 pagesPol Science ProjectAnshu SharmaNo ratings yet
- 52 Blower StoryDocument7 pages52 Blower StoryBentley SpottingNo ratings yet