You might also like
- Discharge SummaryDocument5 pagesDischarge SummarySriram SuryaNo ratings yet
- Blood Component Therapy - TMDocument62 pagesBlood Component Therapy - TMRejwanur Rahman MirazNo ratings yet
- ANP RAM Sepsis ModuleDocument56 pagesANP RAM Sepsis ModuleRyan CracknellNo ratings yet
- Leia Knight 1 PDFDocument3 pagesLeia Knight 1 PDFAnonymous enET0WdPNo ratings yet
- Twin Anemia Polycythemia SyndromesDocument67 pagesTwin Anemia Polycythemia SyndromesBhupendra GuptaNo ratings yet
- Makassed Experience in Management of Placenta AccretaDocument39 pagesMakassed Experience in Management of Placenta AccretaRaluca HabaNo ratings yet
- Nrg203: Care of Mother, Child, and Adolescent: (StudentDocument6 pagesNrg203: Care of Mother, Child, and Adolescent: (Studentmikhaela sencilNo ratings yet
- Role of Modified B-Lynch Suture in Atonic PPH in Cesarean SectionDocument23 pagesRole of Modified B-Lynch Suture in Atonic PPH in Cesarean SectionBagus Arya MahartaNo ratings yet
- General Data and Chief ComplaintDocument21 pagesGeneral Data and Chief ComplaintAyen FornollesNo ratings yet
- The PatientDocument9 pagesThe PatientJan Crizza Dale R. FrancoNo ratings yet
- Major Liver Resection PIN IKABDI Bali 4 Okt 2014 711DFDocument32 pagesMajor Liver Resection PIN IKABDI Bali 4 Okt 2014 711DFElandha PutriNo ratings yet
- Cardiogenic Shock Monitoring and SupportDocument30 pagesCardiogenic Shock Monitoring and SupportFikriYTNo ratings yet
- MODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsDocument7 pagesMODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsalliahjaneadlawanNo ratings yet
- Sepsis: ManagementDocument50 pagesSepsis: Managementer bcmNo ratings yet
- Case Presentation on a 4-Day Old Baby with Fever, Refusal to Feed and Excessive CryDocument34 pagesCase Presentation on a 4-Day Old Baby with Fever, Refusal to Feed and Excessive CrymehwishNo ratings yet
- The CaseDocument33 pagesThe CasemarunxNo ratings yet
- MR Sindrom Nefrotik 1 Agustus 17Document12 pagesMR Sindrom Nefrotik 1 Agustus 17Ridho CahyaNo ratings yet
- MujeebDocument2 pagesMujeebMujb RehmanNo ratings yet
- Groups 3 5 and 6 CasesDocument29 pagesGroups 3 5 and 6 CasesTrishaNo ratings yet
- Duty Report Highlights Patient CaseDocument4 pagesDuty Report Highlights Patient CaseCristian RajagukgukNo ratings yet
- APRIL MORBIDITY AND MORTALITY CASE CONFERENCE: KAWASAKI DISEASEDocument30 pagesAPRIL MORBIDITY AND MORTALITY CASE CONFERENCE: KAWASAKI DISEASEAyen FornollesNo ratings yet
- Increased D-dimer and CRP in Asymptomatic COVID-19 PatientDocument11 pagesIncreased D-dimer and CRP in Asymptomatic COVID-19 PatientYulius TimotiusNo ratings yet
- MORNING REPORT: 3 NEW INPATIENTS AND 2 CONSULTATIONSDocument17 pagesMORNING REPORT: 3 NEW INPATIENTS AND 2 CONSULTATIONSmagda SiraitNo ratings yet
- Non POMR 22 Oktober 2019Document19 pagesNon POMR 22 Oktober 2019magda SiraitNo ratings yet
- Acute Exacerbation of COPDDocument33 pagesAcute Exacerbation of COPDRalphE.BouDeleh100% (1)
- Care 360Document3 pagesCare 360t38dddNo ratings yet
- Case Report Uterine InversionDocument64 pagesCase Report Uterine InversionFelicia Yumita Winata100% (1)
- Sertifikat PIT 7 IDI Kab Sukabumi 2023 Dr. Galih SuharnoDocument2 pagesSertifikat PIT 7 IDI Kab Sukabumi 2023 Dr. Galih Suharnogalih29No ratings yet
- Kasus - I Wayan Aryanta PutraDocument20 pagesKasus - I Wayan Aryanta PutraDiana BaagilNo ratings yet
- MR DOC KAD DR HeriDocument16 pagesMR DOC KAD DR HeriIffaNo ratings yet
- 14 MR Er Krs RDG ZakDocument15 pages14 MR Er Krs RDG Zaktriska antonyNo ratings yet
- Blood Bank SectionDocument6 pagesBlood Bank SectionSamanthaCadaDevillaNo ratings yet
- Deresuscitation ARDSDocument28 pagesDeresuscitation ARDSSudaryadiNo ratings yet
- DR Leonar, DENGUE PIN PAPDI 2019Document51 pagesDR Leonar, DENGUE PIN PAPDI 2019Yuni Purnama SariNo ratings yet
- Postpartum HemmorhageDocument9 pagesPostpartum Hemmorhagechloepaxton030No ratings yet
- Laporan Mingguan Unit Gawat Darurat Kamar BersalinDocument6 pagesLaporan Mingguan Unit Gawat Darurat Kamar BersalinaldoNo ratings yet
- Kuliah 8. Anestesi - Syok Dan Tata LaksananyaDocument63 pagesKuliah 8. Anestesi - Syok Dan Tata LaksananyaDesi Suryani DewiNo ratings yet
- Ahmad Basori VidiDocument30 pagesAhmad Basori VidiIka AyuNo ratings yet
- Nicu FinalDocument3 pagesNicu FinalShylaja LukoseNo ratings yet
- SPMC 1 PDFDocument62 pagesSPMC 1 PDFJ.m.RahulNo ratings yet
- Isaac Typhoid NegativeDocument5 pagesIsaac Typhoid Negativeganesh khondeNo ratings yet
- RLE: Prenatal Care RecordDocument5 pagesRLE: Prenatal Care RecordLovely GurreaNo ratings yet
- Vital Signs & Physical Exam: 9 Month Old Boy with Dengue Hemorrhagic FeverDocument16 pagesVital Signs & Physical Exam: 9 Month Old Boy with Dengue Hemorrhagic FeverSannita Mayusda BadiriNo ratings yet
- CaseDocument13 pagesCasesufiya fatimaNo ratings yet
- Dharmedar SinghDocument2 pagesDharmedar SinghAviral Pratap Singh -4 CNo ratings yet
- Mapping Aqsa 2 RABU PAGI, 14 Juni 2024Document11 pagesMapping Aqsa 2 RABU PAGI, 14 Juni 2024Caesar RiayatsyahNo ratings yet
- Laporan Alat Lt. 8 Dinas Sore 10 Juli 2023 - 1Document15 pagesLaporan Alat Lt. 8 Dinas Sore 10 Juli 2023 - 15gvqzbztqkNo ratings yet
- Apat 2Document4 pagesApat 2rendererichmadarangNo ratings yet
- Saturday, December 5th, 2015Document3 pagesSaturday, December 5th, 2015KaniNo ratings yet
- DM Clinical Meet: Presenter: DR Manish Taneja Moderator: DR S VenkataseshanDocument50 pagesDM Clinical Meet: Presenter: DR Manish Taneja Moderator: DR S Venkataseshanvishal sidanaNo ratings yet
- Penilaian Risiko Anestesi & PembedahanDocument12 pagesPenilaian Risiko Anestesi & PembedahanRyzaAmirethaSaniNo ratings yet
- Template Duty ReportDocument6 pagesTemplate Duty ReportJefri SusantoNo ratings yet
- Panduan Tata Laksana Lesi Pra Kanker ServiksDocument76 pagesPanduan Tata Laksana Lesi Pra Kanker ServiksHandy PutraNo ratings yet
- Report 3Document7 pagesReport 3Souvik DuttaNo ratings yet
- Wkcase FINAL PresentationDocument51 pagesWkcase FINAL Presentationwende kassahunNo ratings yet
- April 2017Document21 pagesApril 2017drpinnakavamsiNo ratings yet
- Megha 2Document5 pagesMegha 2gargrajeshindiaNo ratings yet
- MR Tengah Incovit - Ketut - 240621 - Covid Severe + DMDocument23 pagesMR Tengah Incovit - Ketut - 240621 - Covid Severe + DMDr. Surya Abadi KristyoadiNo ratings yet
- Hosp WA Dec 16 PDFDocument9 pagesHosp WA Dec 16 PDFhanselMD50% (2)
- Medical Notes Interview SPADocument60 pagesMedical Notes Interview SPAhanselMDNo ratings yet
- AwarenessDocument49 pagesAwarenesshanselMDNo ratings yet
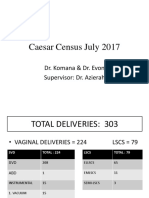
- Caesar Census July 2017Document71 pagesCaesar Census July 2017hanselMDNo ratings yet
- Cerebral ProtectionDocument51 pagesCerebral ProtectionhanselMD100% (1)
- Rapid Sequence InductionDocument8 pagesRapid Sequence InductionAngela Mitchelle NyanganNo ratings yet
- Medication Error Reporting Form Pindaan 2Document2 pagesMedication Error Reporting Form Pindaan 2hanselMD100% (2)
- 221 Smoking and AnaesthesiaDocument4 pages221 Smoking and AnaesthesiaLee June Lyng100% (1)
- M. Med Anaesthesiology Training Programme - Informationfor Medical OfficersDocument3 pagesM. Med Anaesthesiology Training Programme - Informationfor Medical OfficershanselMDNo ratings yet
- Breech PravinDocument39 pagesBreech PravinhanselMDNo ratings yet
- 23 ContraceptionDocument4 pages23 ContraceptionhanselMDNo ratings yet
- 25ECTOPICDocument4 pages25ECTOPIChanselMDNo ratings yet
- Appendix 2: List of High Alert MedicationDocument7 pagesAppendix 2: List of High Alert MedicationhanselMDNo ratings yet
- Molar PregnancyDocument4 pagesMolar PregnancyhanselMD100% (1)
- Gordon'S Functional Health PatternDocument10 pagesGordon'S Functional Health PatternDave SapladNo ratings yet
- Sterility and Its TreaerrrtmentDocument11 pagesSterility and Its TreaerrrtmentFares EL DeenNo ratings yet
- How staying up late affects your sleep and healthDocument16 pagesHow staying up late affects your sleep and healthHelder BalantaNo ratings yet
- Dental Hygiene Resume - No ReferencesDocument2 pagesDental Hygiene Resume - No Referencesapi-313829416No ratings yet
- Histology Report 10-06-2022Document2 pagesHistology Report 10-06-2022chloedee30No ratings yet
- Guidelines For COVID-19Document13 pagesGuidelines For COVID-19Pherdaus Islam AlaminNo ratings yet
- CPE5601 Diagnosis and Treatment of Feeding and Eating DisordersDocument16 pagesCPE5601 Diagnosis and Treatment of Feeding and Eating DisordersSiti MuslihaNo ratings yet
- Volunteer Handbook 2019Document12 pagesVolunteer Handbook 2019Katharine Tondra100% (1)
- Aubf Lab 7Document1 pageAubf Lab 7Regina SalazarNo ratings yet
- 10.1007@s11065 020 09443 7Document14 pages10.1007@s11065 020 09443 7José NettoNo ratings yet
- The Natural Way To A Healthy HealingDocument111 pagesThe Natural Way To A Healthy HealingAnjanaNo ratings yet
- Molar PregnancyDocument5 pagesMolar Pregnancycwqdtgtf6hNo ratings yet
- Atrial Septal Defect (ASD) : For EducatorsDocument7 pagesAtrial Septal Defect (ASD) : For EducatorsJaven BNo ratings yet
- Lifelong Learning of the Elderly in JapanDocument6 pagesLifelong Learning of the Elderly in JapanAzida AlzahariNo ratings yet
- Third Periodic TestDocument5 pagesThird Periodic TestMarry Jane Lustre CanabalNo ratings yet
- Sister Callista RoyDocument17 pagesSister Callista RoyAbhee CalimagNo ratings yet
- UKFP 2024 Applicant HandbookDocument20 pagesUKFP 2024 Applicant HandbookS Abi GunnamNo ratings yet
- Dakota Horizons BrochureDocument2 pagesDakota Horizons Brochurekatie_krebsbach_1No ratings yet
- A. Historical Perspectives: Women's RolesDocument11 pagesA. Historical Perspectives: Women's RolesJoanne SarzonaNo ratings yet
- Component Extension for SAP EHS ManagementDocument103 pagesComponent Extension for SAP EHS ManagementChaitanya NarreddyNo ratings yet
- Borderline Personality Disorder: ? Inadequate Information 1 Absent or False 2 Subthreshold 3 Threshold or TrueDocument4 pagesBorderline Personality Disorder: ? Inadequate Information 1 Absent or False 2 Subthreshold 3 Threshold or Truemarinescu_alexandraNo ratings yet
- Mental: Your Health MattersDocument2 pagesMental: Your Health MattersKrsnaPentayahNo ratings yet
- Different Approaches in Pharmacological ResearchDocument3 pagesDifferent Approaches in Pharmacological ResearcharcherselevatorsNo ratings yet
- Briefing Note: Elite Victimization of ChildrenDocument8 pagesBriefing Note: Elite Victimization of ChildrenEdNo ratings yet
- Foodborne IllnessDocument18 pagesFoodborne IllnesspaanarNo ratings yet
- Healthy Eating HabitsDocument24 pagesHealthy Eating HabitsRyan ReyesNo ratings yet
- Ethical Principle S: Joy Lyzette Reguyal Carreon, RN, ManDocument26 pagesEthical Principle S: Joy Lyzette Reguyal Carreon, RN, ManRomelyn Duque DellomesNo ratings yet
- Week 4 (February 14 - 19) System Life CycleDocument9 pagesWeek 4 (February 14 - 19) System Life CycleChrisanta Joyce Dela Cruz BOCALIGNo ratings yet
- Ncp. Pedia.Document2 pagesNcp. Pedia.Czarina MayoNo ratings yet
- Domperidone For Increasing Breast Milk Supply 260219 PDFDocument2 pagesDomperidone For Increasing Breast Milk Supply 260219 PDFANneNo ratings yet
- Brain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfFrom EverandBrain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfRating: 5 out of 5 stars5/5 (2)
- What to Expect When You’re Expecting (5th Edition)From EverandWhat to Expect When You’re Expecting (5th Edition)Rating: 5 out of 5 stars5/5 (1)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeFrom EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeRating: 3.5 out of 5 stars3.5/5 (13)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- What No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodFrom EverandWhat No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodRating: 4.5 out of 5 stars4.5/5 (30)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenFrom EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenRating: 4 out of 5 stars4/5 (153)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodFrom EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodRating: 5 out of 5 stars5/5 (33)
- Period Power: Harness Your Hormones and Get Your Cycle Working For YouFrom EverandPeriod Power: Harness Your Hormones and Get Your Cycle Working For YouRating: 4 out of 5 stars4/5 (25)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeFrom EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNo ratings yet
- The Menopause Manifesto: Own Your Health With Facts and FeminismFrom EverandThe Menopause Manifesto: Own Your Health With Facts and FeminismRating: 4 out of 5 stars4/5 (18)
- Skinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!From EverandSkinny Bitch: A No-Nonsense, Tough-Love Guide for Savvy Girls Who Want to Stop Eating Crap and Start Looking Fabulous!Rating: 3.5 out of 5 stars3.5/5 (488)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersFrom EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersRating: 4.5 out of 5 stars4.5/5 (71)
- The 21-Day Self-Love Challenge: Learn How to Love Yourself Unconditionally, Cultivate Confidence, Self-Compassion and Self-WorthFrom EverandThe 21-Day Self-Love Challenge: Learn How to Love Yourself Unconditionally, Cultivate Confidence, Self-Compassion and Self-WorthNo ratings yet
- Younger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondFrom EverandYounger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondRating: 4 out of 5 stars4/5 (110)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- The Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthFrom EverandThe Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthRating: 4.5 out of 5 stars4.5/5 (21)
- The Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysFrom EverandThe Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysRating: 4.5 out of 5 stars4.5/5 (5)
- I'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeFrom EverandI'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeRating: 4 out of 5 stars4/5 (15)
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionFrom EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionRating: 4.5 out of 5 stars4.5/5 (124)
- The Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesFrom EverandThe Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesNo ratings yet
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondFrom EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondRating: 4.5 out of 5 stars4.5/5 (38)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayFrom EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayRating: 5 out of 5 stars5/5 (2)
- The First Forty Days: The Essential Art of Nourishing the New MotherFrom EverandThe First Forty Days: The Essential Art of Nourishing the New MotherRating: 5 out of 5 stars5/5 (5)
- The Path of the Priestess: A Guidebook for Awakening the Divine FeminineFrom EverandThe Path of the Priestess: A Guidebook for Awakening the Divine FeminineRating: 4 out of 5 stars4/5 (2)
- Dark Feminine Energy: Free Your Femme Fatale Ignite Your Irresistible Allure Through Mystique, Sexuality, Femininity, and Elegance to Become the Dark Diva No One Can IgnoreFrom EverandDark Feminine Energy: Free Your Femme Fatale Ignite Your Irresistible Allure Through Mystique, Sexuality, Femininity, and Elegance to Become the Dark Diva No One Can IgnoreRating: 1 out of 5 stars1/5 (1)
- Mayo Clinic Guide To A Healthy Pregnancy, 2nd EditionFrom EverandMayo Clinic Guide To A Healthy Pregnancy, 2nd EditionRating: 4.5 out of 5 stars4.5/5 (7)
- Perimenopause Power: Navigating your hormones on the journey to menopauseFrom EverandPerimenopause Power: Navigating your hormones on the journey to menopauseRating: 4 out of 5 stars4/5 (2)
- Sacred Womb Healing Meditation Divine feminine alignment: heal ancestral traumas deep wounds, release blocked sexual energies, flow to creativity, overcome the energies of birthing, joy love happyFrom EverandSacred Womb Healing Meditation Divine feminine alignment: heal ancestral traumas deep wounds, release blocked sexual energies, flow to creativity, overcome the energies of birthing, joy love happyRating: 5 out of 5 stars5/5 (1)
- The Radium Girls: The Dark Story of America's Shining Women (Harrowing Historical Nonfiction Bestseller About a Courageous Fight for Justice)From EverandThe Radium Girls: The Dark Story of America's Shining Women (Harrowing Historical Nonfiction Bestseller About a Courageous Fight for Justice)Rating: 4 out of 5 stars4/5 (945)