You might also like
- Gujarat Gas: CMP: INR407 Strong As A Hulk!Document8 pagesGujarat Gas: CMP: INR407 Strong As A Hulk!dashNo ratings yet
- Climate Change and Its Impact (CCI-2023) Climate Change and Its Impact (CCI-2023)Document9 pagesClimate Change and Its Impact (CCI-2023) Climate Change and Its Impact (CCI-2023)hksachinNo ratings yet
- Who Vacination Requirments and Health AdviceDocument100 pagesWho Vacination Requirments and Health AdviceHasancan YavaşNo ratings yet
- Firm Culture and Leadership as Predictors of Firm PerformanceDocument6 pagesFirm Culture and Leadership as Predictors of Firm Performancechernet kebedeNo ratings yet
- Kotak Group Smart Cash: Certificate of InsuranceDocument3 pagesKotak Group Smart Cash: Certificate of InsuranceHeishnam SinghNo ratings yet
- JULI 2022 OBAT PERENCAAN DATADocument1,260 pagesJULI 2022 OBAT PERENCAAN DATAsanti susantiNo ratings yet
- Mint Delhi 28-10-2022Document20 pagesMint Delhi 28-10-2022sushilpal161No ratings yet
- NOTES CD Lecture Generic 2022Document182 pagesNOTES CD Lecture Generic 2022Meryville JacildoNo ratings yet
- On Screen Writing BookDocument61 pagesOn Screen Writing BookDada DadaNo ratings yet
- Đề T.AnhDocument17 pagesĐề T.AnhMai Phạm0% (1)
- Mindworkzz Formulae SheetDocument66 pagesMindworkzz Formulae SheetDeepak MNo ratings yet
- Amrita Sher-Gil ReaderDocument19 pagesAmrita Sher-Gil Readersandip luisNo ratings yet
- Management Mandible ReconstructionsDocument32 pagesManagement Mandible ReconstructionsHidayatNo ratings yet
- Suggested Answer CAP II Dec 2013 8Document91 pagesSuggested Answer CAP II Dec 2013 8Dipen AdhikariNo ratings yet
- Solid State Physics LaboratoryDocument41 pagesSolid State Physics LaboratoryMOHIT PARASHARNo ratings yet
- Odisha Current Affairs Questions and AnswersDocument145 pagesOdisha Current Affairs Questions and AnswersJayanta mendiliNo ratings yet
- PCWB-2316 FLXL Black N100-IdDocument4 pagesPCWB-2316 FLXL Black N100-IdFindora InternusaNo ratings yet
- Pass ListDocument2 pagesPass Listsabin dangolNo ratings yet
- Vision Fitness T9550 Treadmill Assembly InstructionsDocument8 pagesVision Fitness T9550 Treadmill Assembly InstructionspkrajniNo ratings yet
- SOP - SDF For Regional Tourists - V13 (Approved by The Cabinet)Document6 pagesSOP - SDF For Regional Tourists - V13 (Approved by The Cabinet)Tenzin TsheltrimNo ratings yet
- Bitcoin Price Prediction Using Machine Learning: Presented byDocument24 pagesBitcoin Price Prediction Using Machine Learning: Presented byHarshNo ratings yet
- Shoe Shop Management System ProjectDocument34 pagesShoe Shop Management System Projectshubham kumarNo ratings yet
- 1896-Article Text-7540-1-10-20220308Document13 pages1896-Article Text-7540-1-10-20220308International Health ReviewNo ratings yet
- Lab 5 Report: Đại học Duy Tân Khoa Điện - Điện tửDocument22 pagesLab 5 Report: Đại học Duy Tân Khoa Điện - Điện tửNhân HồNo ratings yet
- Czab 133Document9 pagesCzab 1337 MNTNo ratings yet
- Catalogue Brand Book 2022Document32 pagesCatalogue Brand Book 2022Rifqi Athallah (Mickey James)No ratings yet
- The I Newspaper - Issue 3743 (22 Nov 2022)Document56 pagesThe I Newspaper - Issue 3743 (22 Nov 2022)Me4MeNo ratings yet
- CGL 2020 candidates allocated to postal circlesDocument2 pagesCGL 2020 candidates allocated to postal circlesAMIT TIWARINo ratings yet
- Chevrolet Corvette (C6)Document12 pagesChevrolet Corvette (C6)robertoNo ratings yet
- FASH235 Document 2Document2 pagesFASH235 Document 2siibnuNo ratings yet
- Universal Gravitational Constant: EquipmentDocument13 pagesUniversal Gravitational Constant: EquipmentTraitor OneNo ratings yet
- Apply for PISIC WAH trainingDocument2 pagesApply for PISIC WAH trainingSuresh KannanNo ratings yet
- Digested Journal#7Document4 pagesDigested Journal#7Jay Raymond DelfinNo ratings yet
- 924 3184 2 PBDocument8 pages924 3184 2 PBRestiana Antonia PutriNo ratings yet
- UnlockedDocument30 pagesUnlockedAvinitsahaNo ratings yet
- Ws 604Document21 pagesWs 604Enoc Alexander Gelabert CornielleNo ratings yet
- Online Grocery ShopDocument6 pagesOnline Grocery ShopIJRASETPublicationsNo ratings yet
- Recount TextDocument9 pagesRecount TextHeldaNo ratings yet
- New Hire TrainingDocument37 pagesNew Hire TrainingEdward MarquezNo ratings yet
- PS/Consolidated Premium Statement /ver 2.1/jan 2021: A Reliance Capital CompanyDocument1 pagePS/Consolidated Premium Statement /ver 2.1/jan 2021: A Reliance Capital CompanyJhansi RokatiNo ratings yet
- Practice+Costing+Card+ +Garden+SaladDocument4 pagesPractice+Costing+Card+ +Garden+Saladみなと あかりNo ratings yet
- Seleccion of Regressors in Econometrics Non Parametrics & Parametrics Methods - LavergneDocument48 pagesSeleccion of Regressors in Econometrics Non Parametrics & Parametrics Methods - LavergneFranciscoNo ratings yet
- Hindi 4Document140 pagesHindi 4Debnath SahaNo ratings yet
- Transcription+ +S1+ +Demand+and+Supply+Document15 pagesTranscription+ +S1+ +Demand+and+Supply+Sonu KumarNo ratings yet
- Retraction Hooks of Different Lengths For Maxillary Whole Arch Distalization With Miniscrew Anchorage: A Finite Element AnalysisDocument14 pagesRetraction Hooks of Different Lengths For Maxillary Whole Arch Distalization With Miniscrew Anchorage: A Finite Element AnalysisKanchit SuwanswadNo ratings yet
- Standards For Trade BDDocument3 pagesStandards For Trade BDRasel777No ratings yet
- Samsung Tv8Document65 pagesSamsung Tv8Enrile Labiano BaduaNo ratings yet
- BYKPT2196M 14 09 2022 09 - 53 - 05 - UnDocument52 pagesBYKPT2196M 14 09 2022 09 - 53 - 05 - UnHani AjmalNo ratings yet
- CH 7 StudyonenzymatictreatmentforbiosofteningDocument46 pagesCH 7 StudyonenzymatictreatmentforbiosofteningAnanya SinghNo ratings yet
- 16 January, 2023Document1 page16 January, 2023himdrive 69No ratings yet
- 07 - C-Leg - Power ManagementDocument11 pages07 - C-Leg - Power ManagementSalemNo ratings yet
- List Price W.E.F. 28 Oct., 2020Document8 pagesList Price W.E.F. 28 Oct., 2020chaitanyaomronNo ratings yet
- OD126164812918973000Document1 pageOD126164812918973000Manoj SirsatNo ratings yet
- Bond Overview 1 PDFDocument6 pagesBond Overview 1 PDFAkash SinghNo ratings yet
- Hur FashionDocument50 pagesHur FashionRashan Jida ReshanNo ratings yet
- Adaptive Spatial Image Steganography and Steganalysis Using Perceptual Modelling and Machine LearningDocument189 pagesAdaptive Spatial Image Steganography and Steganalysis Using Perceptual Modelling and Machine LearningDemaZiad100% (1)
- Mathematics: CatalogueDocument16 pagesMathematics: CatalogueVandana Tiwari0% (1)
- Technical Data Sheet Chemitac 23: DescriptionDocument3 pagesTechnical Data Sheet Chemitac 23: DescriptionPhuong The NguyenNo ratings yet
- RegUpdate26 APFDocument10 pagesRegUpdate26 APFEverly Alves caetanoNo ratings yet
- POMR FAH BAshori CMLDocument22 pagesPOMR FAH BAshori CMLIka AyuNo ratings yet
- Cue and Clue PL Idx PDX PTX Pmo&Ed: Mrs. C /79 Yo/Incovit Ward Subjective Non PharmacologyDocument12 pagesCue and Clue PL Idx PDX PTX Pmo&Ed: Mrs. C /79 Yo/Incovit Ward Subjective Non PharmacologyIka AyuNo ratings yet
- Gestational Diabetes Mellitus (GDM), Diagnostics, Therapy 2021Document11 pagesGestational Diabetes Mellitus (GDM), Diagnostics, Therapy 2021Ika AyuNo ratings yet
- Toxins: Cardiotoxicity of Uremic Toxins: A Driver of Cardiorenal SyndromeDocument29 pagesToxins: Cardiotoxicity of Uremic Toxins: A Driver of Cardiorenal SyndromeIka AyuNo ratings yet
- Management of Diabetes in Pregnancy ADA 2022Document12 pagesManagement of Diabetes in Pregnancy ADA 2022Ika AyuNo ratings yet
- Morning Report: Physician in ChargeDocument33 pagesMorning Report: Physician in ChargeIka AyuNo ratings yet
- Morning Report: Dr. Reza's PatientsDocument24 pagesMorning Report: Dr. Reza's PatientsIka AyuNo ratings yet
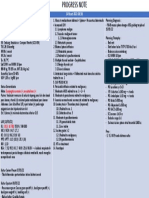
- Progress Note for Patient with Mediastinal and Abdominal MassesDocument1 pageProgress Note for Patient with Mediastinal and Abdominal MassesIka AyuNo ratings yet
- Diverticular Disease: - Diverticulosis - DiverticulitisDocument14 pagesDiverticular Disease: - Diverticulosis - DiverticulitisIka AyuNo ratings yet
- Recommendations On Screening For Colorectal Cancer 2016: Canadian Task Force On Preventive Health Care (CTFPHC)Document38 pagesRecommendations On Screening For Colorectal Cancer 2016: Canadian Task Force On Preventive Health Care (CTFPHC)Ika AyuNo ratings yet
- Medical Consultation From Neurology Department: The Aim of ConsultationDocument19 pagesMedical Consultation From Neurology Department: The Aim of ConsultationIka AyuNo ratings yet
- AYU - CKD+DVT Left ArmDocument25 pagesAYU - CKD+DVT Left ArmIka AyuNo ratings yet
- Sequential Therapy For Hepatocellular Carcinoma AfDocument9 pagesSequential Therapy For Hepatocellular Carcinoma AfIka AyuNo ratings yet
- Wei Wang's Research on Combating Neglected Tropical DiseasesDocument14 pagesWei Wang's Research on Combating Neglected Tropical DiseasesIka AyuNo ratings yet
- Diverticular Disease of The Colon: Jason Phillips, MDDocument73 pagesDiverticular Disease of The Colon: Jason Phillips, MDfarhan adiNo ratings yet
- POMR FAH BAshori CMLDocument22 pagesPOMR FAH BAshori CMLIka AyuNo ratings yet
- Sos Pomr SatitiDocument30 pagesSos Pomr SatitiIka AyuNo ratings yet
- Heteroanamnesa Chief Complaint: Coffe Ground Vomiting History of Present IllnessDocument6 pagesHeteroanamnesa Chief Complaint: Coffe Ground Vomiting History of Present IllnessIka AyuNo ratings yet
- POMR Satiti Acute CholangitisDocument30 pagesPOMR Satiti Acute CholangitisIka AyuNo ratings yet
- Mr. Y A S / 49 Y.o/ Ward Chief Complaint: Lump in Chest History of Present IllnessDocument31 pagesMr. Y A S / 49 Y.o/ Ward Chief Complaint: Lump in Chest History of Present IllnessIka AyuNo ratings yet
- Summary of Patient Database RecordDocument21 pagesSummary of Patient Database RecordIka AyuNo ratings yet
- Cue and Clue PL Idx PDX PTX Pmo&Ed: Mr. T/86Yo/ Ward 26 Subjective Non PharmacologyDocument8 pagesCue and Clue PL Idx PDX PTX Pmo&Ed: Mr. T/86Yo/ Ward 26 Subjective Non PharmacologyIka AyuNo ratings yet
- Database Summary of 17-Year-Old Male with Leg SwellingDocument27 pagesDatabase Summary of 17-Year-Old Male with Leg SwellingIka AyuNo ratings yet
- Program Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaDocument17 pagesProgram Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaIka AyuNo ratings yet
- POMR Satiti Medical ConsultationDocument18 pagesPOMR Satiti Medical ConsultationIka AyuNo ratings yet
- Mrs. I/ 38 Y.o/ w.8 Chief Complaint: History of Present IllnessDocument19 pagesMrs. I/ 38 Y.o/ w.8 Chief Complaint: History of Present IllnessIka AyuNo ratings yet
- Managing Hyperglycemia in STEMI PatientDocument18 pagesManaging Hyperglycemia in STEMI PatientIka AyuNo ratings yet
- Program Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaDocument27 pagesProgram Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaIka AyuNo ratings yet
- Sos Kimesej ManDocument14 pagesSos Kimesej ManIka AyuNo ratings yet
- POMR Medical Record for Metabolic Acidosis PatientDocument5 pagesPOMR Medical Record for Metabolic Acidosis PatientIka AyuNo ratings yet
- 2010 HSC Exam PhysicsDocument42 pages2010 HSC Exam PhysicsVictor345No ratings yet
- Simulia Abaqus Standard DatasheetDocument3 pagesSimulia Abaqus Standard Datasheetuser923019231831No ratings yet
- FM 5130Document66 pagesFM 5130Aswini Kr KarmakarNo ratings yet
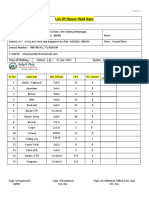
- List of household items for relocationDocument4 pagesList of household items for relocationMADDYNo ratings yet
- Chronological OrderDocument5 pagesChronological OrderDharWin d'Wing-Wing d'AriestBoyzNo ratings yet
- Openness To Experience: Intellect & Openness: Lecture Notes 8Document8 pagesOpenness To Experience: Intellect & Openness: Lecture Notes 8Danilo Pesic100% (1)
- TNG UPDATE InstructionsDocument10 pagesTNG UPDATE InstructionsDiogo Alexandre Crivelari CrivelNo ratings yet
- EPISIOTOMYDocument17 pagesEPISIOTOMYKaye Arriane TenorioNo ratings yet
- Plastic Welding: We Know HowDocument125 pagesPlastic Welding: We Know Howprabal rayNo ratings yet
- Bhakti Trader Ram Pal JiDocument232 pagesBhakti Trader Ram Pal JiplancosterNo ratings yet
- 2 5 Marking ScheduleDocument6 pages2 5 Marking Scheduleapi-218511741No ratings yet
- Managing Post COVID SyndromeDocument4 pagesManaging Post COVID SyndromeReddy VaniNo ratings yet
- GKInvest Market ReviewDocument66 pagesGKInvest Market ReviewjhonxracNo ratings yet
- Delhi (The Capital of India) : Ebook by Ssac InstituteDocument27 pagesDelhi (The Capital of India) : Ebook by Ssac InstituteAnanjay ChawlaNo ratings yet
- GD&T WIZ Tutor Covers The Vast Breadth of Geometric Dimensioning and Tolerancing Without Compromising On The Depth. The Topics Covered AreDocument1 pageGD&T WIZ Tutor Covers The Vast Breadth of Geometric Dimensioning and Tolerancing Without Compromising On The Depth. The Topics Covered AreVinay ManjuNo ratings yet
- Document-SAP EWM For Fashion 1.0: 1.general IntroductionDocument3 pagesDocument-SAP EWM For Fashion 1.0: 1.general IntroductionAnonymous u3PhTjWZRNo ratings yet
- Design & Construction of Substation 16P Painting System ComplianceDocument103 pagesDesign & Construction of Substation 16P Painting System ComplianceRamil LazNo ratings yet
- Building Primitive Traps & SnaresDocument101 pagesBuilding Primitive Traps & SnaresJoseph Madr90% (10)
- TNTCL Cost Data 2021 22Document95 pagesTNTCL Cost Data 2021 22Akd DeshmukhNo ratings yet
- Mechanical Engineer with Experience in Heavy Mining Machinery MaintenanceDocument1 pageMechanical Engineer with Experience in Heavy Mining Machinery MaintenanceCertified Rabbits LoverNo ratings yet
- ProjectDocument86 pagesProjectrajuNo ratings yet
- Second Quarterly Examination Math 9Document2 pagesSecond Quarterly Examination Math 9Mark Kiven Martinez94% (16)
- BCRW Course - Answer-Booklet PDFDocument18 pagesBCRW Course - Answer-Booklet PDFSarah ChaudharyNo ratings yet
- European Business in China Position Paper 2017 2018 (English Version)Document408 pagesEuropean Business in China Position Paper 2017 2018 (English Version)Prasanth RajuNo ratings yet
- Scientology Abridged Dictionary 1973Document21 pagesScientology Abridged Dictionary 1973Cristiano Manzzini100% (2)
- IPO Fact Sheet - Accordia Golf Trust 140723Document4 pagesIPO Fact Sheet - Accordia Golf Trust 140723Invest StockNo ratings yet
- Barcelona Smart City TourDocument44 pagesBarcelona Smart City TourPepe JeansNo ratings yet
- Olympic Ayres Magic LyricsDocument1 pageOlympic Ayres Magic Lyricsjackliddy96No ratings yet
- Project Report Software and Web Development Company: WWW - Dparksolutions.inDocument12 pagesProject Report Software and Web Development Company: WWW - Dparksolutions.inRavi Kiran Rajbhure100% (1)
- 13Document47 pages13Rohan TirmakheNo ratings yet