You might also like
- Management of Acne: Dr. (Sqn. LDR.) V. K. Upadhyaya Head Dept. of Dermatology Pushpanjali Crosslay HospitalDocument48 pagesManagement of Acne: Dr. (Sqn. LDR.) V. K. Upadhyaya Head Dept. of Dermatology Pushpanjali Crosslay HospitalPushpanjali Crosslay HospitalNo ratings yet
- Acne: Acne Treatment: Acne Removal: Acne Remedies For Clear SkinFrom EverandAcne: Acne Treatment: Acne Removal: Acne Remedies For Clear SkinNo ratings yet
- Acne Vulgaris: Cynthia Salinas, M.D. PGY-3 Patient Conference February 2, 2005Document29 pagesAcne Vulgaris: Cynthia Salinas, M.D. PGY-3 Patient Conference February 2, 2005Agnes NesiaNo ratings yet
- 0502 AcneDocument29 pages0502 AcneSam ShahbazNo ratings yet
- Explain AcneDocument3 pagesExplain Acnejoseph curranNo ratings yet
- AcneDocument33 pagesAcneDr.A.K.M.Zayedul Haque MithunNo ratings yet
- Acne: Evaluation and ManagementDocument46 pagesAcne: Evaluation and ManagementChirra WilliamsNo ratings yet
- Acne: Evaluation and ManagementDocument46 pagesAcne: Evaluation and ManagementPraneethaNo ratings yet
- Acne Vulgaris (Or Acne) Is A CommonDocument21 pagesAcne Vulgaris (Or Acne) Is A CommonNia YuniarNo ratings yet
- Acne Vulgaris PowerpointDocument21 pagesAcne Vulgaris PowerpointEricks Manfun100% (3)
- Training ManualDocument125 pagesTraining ManualNermin El sayed100% (1)
- AcneDocument13 pagesAcneOktiya SariNo ratings yet
- Acne Vulgaris-1Document7 pagesAcne Vulgaris-1amanabduwahabNo ratings yet
- Moorfields Pharmaceuticals Product ListDocument8 pagesMoorfields Pharmaceuticals Product ListsightbdNo ratings yet
- Acne Update Aug 2013 - Lay Reviewed Aug 2013 PDFDocument6 pagesAcne Update Aug 2013 - Lay Reviewed Aug 2013 PDFErika DiannaNo ratings yet
- Jurnal Acne VulgarisDocument20 pagesJurnal Acne VulgarisKatihara BrendaNo ratings yet
- Case Studies From Dermatology WorkshopDocument35 pagesCase Studies From Dermatology Workshopstarn.serventisNo ratings yet
- Neonatal and Infant CareDocument10 pagesNeonatal and Infant CareCarla JimenezNo ratings yet
- Patient Information From BMJ: Last Published: Dec 13, 2018Document4 pagesPatient Information From BMJ: Last Published: Dec 13, 2018Binhbong NguyenNo ratings yet
- Acne Vulgaris With Its Homoeopathic and Different Mode of TreatmentDocument12 pagesAcne Vulgaris With Its Homoeopathic and Different Mode of TreatmentAmreen KausarNo ratings yet
- KenaLeen Cream and VitiligoDocument33 pagesKenaLeen Cream and VitiligoRahma MejriNo ratings yet
- AcneDocument4 pagesAcneAriez ChesterNo ratings yet
- Causes & Treatment: Dr. Tinny Ho, June 29, 2004Document26 pagesCauses & Treatment: Dr. Tinny Ho, June 29, 2004Fitrah Tulijalrezya0% (1)
- Jrsocmed00196 0015 PDFDocument5 pagesJrsocmed00196 0015 PDFxiuhtlaltzinNo ratings yet
- What You Need To Know About AcneDocument5 pagesWhat You Need To Know About AcnerichardgomezNo ratings yet
- Skin OtcDocument53 pagesSkin OtcMai MosaadNo ratings yet
- Acne VulgarisDocument45 pagesAcne VulgarisKeith OmwoyoNo ratings yet
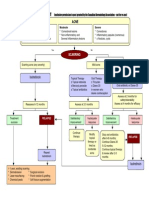
- Flow Chart For Acne Management: IsotretinoinDocument1 pageFlow Chart For Acne Management: IsotretinoinRyan KingNo ratings yet
- Skin Relating Problems: Prepared by Sushmita Rana M PharmDocument36 pagesSkin Relating Problems: Prepared by Sushmita Rana M PharmDRx Sonali TareiNo ratings yet
- How To Use Acne Meds UpdatedDocument4 pagesHow To Use Acne Meds Updatedarmydoc1972No ratings yet
- My Top Ten Menopausal Skin HacksDocument6 pagesMy Top Ten Menopausal Skin Hackslifeinhim100% (1)
- Atopic Dermatitis (Eczema) - Diagnosis and Treatment - Mayo ClinicDocument1 pageAtopic Dermatitis (Eczema) - Diagnosis and Treatment - Mayo ClinicHarry LeNo ratings yet
- Acne Information Society For Pediatric DermatologygownikkkjrDocument2 pagesAcne Information Society For Pediatric Dermatologygownikkkjredwardvault26No ratings yet
- Dermatoterapi CitraDocument46 pagesDermatoterapi CitraKevin BlackNo ratings yet
- Diagnosis and Treatment of AcneDocument8 pagesDiagnosis and Treatment of AcneFreddy PanjaitanNo ratings yet
- TreatmentDocument11 pagesTreatmentsanyassandhuNo ratings yet
- 09 ResurfacingDocument94 pages09 ResurfacingzzmasterNo ratings yet
- How I Cured My Seborrheic Dermatitis NaturallyDocument3 pagesHow I Cured My Seborrheic Dermatitis NaturallyXavier VásquezNo ratings yet
- Acne Vulgaris By: Dr. Majid Suhail Prof DermatologyDocument78 pagesAcne Vulgaris By: Dr. Majid Suhail Prof DermatologyMajid SuhailNo ratings yet
- The Only Guide For Acne Home Remedies, Medication, Types & Scar RemovalDocument2 pagesThe Only Guide For Acne Home Remedies, Medication, Types & Scar Removalbonsaipants40No ratings yet
- What Is The Best Method To Remove Pearly Papules Easily and Quickly at Home in 2019 PDFDocument3 pagesWhat Is The Best Method To Remove Pearly Papules Easily and Quickly at Home in 2019 PDFElizabeth KingsleyNo ratings yet
- Derm Referral Guidelines - Diaper Dermatitis (AC 2018)Document2 pagesDerm Referral Guidelines - Diaper Dermatitis (AC 2018)Marium BanoNo ratings yet
- AcneDocument2 pagesAcnereginaNo ratings yet
- AcneDocument64 pagesAcneMohamed AdelNo ratings yet
- How Is Seborrheic Dermatitis TreatedDocument3 pagesHow Is Seborrheic Dermatitis TreatedDutt DuttNo ratings yet
- AdvicesDocument13 pagesAdvicesrajsekhar sahaNo ratings yet
- Bula Nizoral 3 Paginas OriginalDocument3 pagesBula Nizoral 3 Paginas OriginalAntónio PestanaNo ratings yet
- Chemicals For ConsumersDocument50 pagesChemicals For ConsumersAzie Nurul Akhtar100% (1)
- Acne Vulgaris RevisiDocument34 pagesAcne Vulgaris RevisiTirzalia LianNo ratings yet
- MSDS Petroflo 20y25Document10 pagesMSDS Petroflo 20y25Arie PanjunanNo ratings yet
- Safety Data Sheet: Section 1: Identification of The Product and CompanyDocument7 pagesSafety Data Sheet: Section 1: Identification of The Product and CompanyFuckyouNo ratings yet
- Agatha Thrash Master CompilationDocument1,410 pagesAgatha Thrash Master CompilationCongresso MV100% (7)
- Topical FormulationsDocument5 pagesTopical FormulationsSandeep GargNo ratings yet
- Acid or Bichloroacetic Acid Topical Treatments Can Shrink or Remove The Fordyce Spots. These Work Best in Combination With Laser Treatment.Document2 pagesAcid or Bichloroacetic Acid Topical Treatments Can Shrink or Remove The Fordyce Spots. These Work Best in Combination With Laser Treatment.Kevin ShirlinNo ratings yet
- Who Gets Periorificial DermatitisDocument3 pagesWho Gets Periorificial DermatitismainNo ratings yet
- Zinc OxideDocument4 pagesZinc OxideyundayundaaNo ratings yet
- OTC TableDocument60 pagesOTC TableShamel Eshak75% (4)
- Personalized Advice: Clearing Your AcneDocument8 pagesPersonalized Advice: Clearing Your AcneAsh MizukiNo ratings yet
- Cs 8Document2 pagesCs 8AbdulAzees S DeenmohamedNo ratings yet
- Homeopathic Thesaurus 2016Document274 pagesHomeopathic Thesaurus 2016Tahir Naqvi100% (1)
- Abdo LumpDocument1 pageAbdo LumpAbhijitNo ratings yet
- Peds Proforma N DietDocument2 pagesPeds Proforma N DietAbhijitNo ratings yet
- Cover ThesisDocument6 pagesCover ThesisAbhijitNo ratings yet
- A Homoeopathic Approach To Cancer 1Document29 pagesA Homoeopathic Approach To Cancer 1Salvador Piñeiro Ferradanes100% (3)
- See Your Own Aura in 5 Minutes or LessDocument0 pagesSee Your Own Aura in 5 Minutes or Lessmarija7gregicNo ratings yet
- Constitutional Medicine - John H. ClarkeDocument77 pagesConstitutional Medicine - John H. Clarkemelos24No ratings yet
- MAINwjpps PDFDocument27 pagesMAINwjpps PDFAbhijitNo ratings yet
- Acne VulgarisDocument31 pagesAcne VulgarisAbhijitNo ratings yet
- MEG 05 Assignments 2018 19Document34 pagesMEG 05 Assignments 2018 19ANJAN GOGOINo ratings yet
- Acne: Evaluation and ManagementDocument46 pagesAcne: Evaluation and ManagementChirra WilliamsNo ratings yet
- MethodologyDocument2 pagesMethodologyAbhijitNo ratings yet
- Abstract Squares PowerPoint TemplatesDocument48 pagesAbstract Squares PowerPoint Templatesdwi eriyantoNo ratings yet
- Useful Mother Tinctures in My Homoeopathic PracticeDocument8 pagesUseful Mother Tinctures in My Homoeopathic PracticeAbhijit100% (1)
- Review Article 1Document9 pagesReview Article 1AbhijitNo ratings yet
- List of Homoeopathic Medicines, Combinations & Their UsesDocument29 pagesList of Homoeopathic Medicines, Combinations & Their Usesgirish261187% (55)
- ABOAKNSDocument9 pagesABOAKNSAbhijitNo ratings yet
- Common Cold Flu and HomoeopathyDocument11 pagesCommon Cold Flu and HomoeopathyAbhijitNo ratings yet
- Homeopathic Medicines For Hoarse Voice - Homeopathy TreatmentDocument5 pagesHomeopathic Medicines For Hoarse Voice - Homeopathy TreatmentAbhijitNo ratings yet
- Get Rid of Nocturnal EnurDocument8 pagesGet Rid of Nocturnal EnurAbhijitNo ratings yet
- Common Cold Flu and HomoeopathyDocument11 pagesCommon Cold Flu and HomoeopathyAbhijitNo ratings yet
- Quick RemediesDocument13 pagesQuick RemediesAbhijitNo ratings yet
- Chart of Plant Families and Miasms PDFDocument4 pagesChart of Plant Families and Miasms PDFAbhijitNo ratings yet
- Sankaran's MiasmsDocument46 pagesSankaran's MiasmsHomeopathy Torrents95% (43)
- Constitution: Phosphorus Phos-Ac. SulphurDocument1 pageConstitution: Phosphorus Phos-Ac. SulphurAbhijitNo ratings yet
- Homeopathic Remedies For 'Flu - Flow ChartDocument1 pageHomeopathic Remedies For 'Flu - Flow Chartisadore97% (31)
- Homeopathic Remedies For 'Flu - Flow ChartDocument1 pageHomeopathic Remedies For 'Flu - Flow Chartisadore97% (31)
- IEEE Copyright FormDocument2 pagesIEEE Copyright FormMatías IgnacioNo ratings yet
- Homeopathic Remedies For 'Flu - Flow ChartDocument1 pageHomeopathic Remedies For 'Flu - Flow Chartisadore97% (31)
- Letting Go by Atul GawandeDocument18 pagesLetting Go by Atul Gawandetakoyakilovers100% (2)
- General DeclarationDocument1 pageGeneral DeclarationPos SMB IINo ratings yet
- Sterile TechDocument85 pagesSterile TechBSN II - Tutor, Rel joshuaNo ratings yet
- Nursing NotesDocument6 pagesNursing NotesTiffany SimnickNo ratings yet
- Somatic RecombinationDocument5 pagesSomatic RecombinationNoor Ul NaeemNo ratings yet
- Hematology Unit: Complete Blood Count (CBC)Document2 pagesHematology Unit: Complete Blood Count (CBC)Rasha ElbannaNo ratings yet
- Biology Investigatory Project On Caffeine AddectionDocument5 pagesBiology Investigatory Project On Caffeine AddectionShivam SinghNo ratings yet
- Diagnostic Challenges and Uncertainties of Embolic Strokes of UndeterminedDocument4 pagesDiagnostic Challenges and Uncertainties of Embolic Strokes of UndeterminedDarliana Ospina DuarteNo ratings yet
- Manual of Definitive Surgical Trauma CareDocument256 pagesManual of Definitive Surgical Trauma Carebovine splendor100% (3)
- 2021 Va Ers DataDocument1,788 pages2021 Va Ers DataasdasdasdNo ratings yet
- MCQs in para (With Answers)Document20 pagesMCQs in para (With Answers)janiceli020785% (26)
- ShouldiceDocument16 pagesShouldiceAbdullah AhmedNo ratings yet
- Artificial or Supplimentary FoodDocument4 pagesArtificial or Supplimentary FoodArchana Sahu100% (1)
- Microbiology: Pathogenic Gram-Positive Cocci (Streptococcus)Document26 pagesMicrobiology: Pathogenic Gram-Positive Cocci (Streptococcus)Shuler0071No ratings yet
- CLICO Group Health and Life Coverage 1Document12 pagesCLICO Group Health and Life Coverage 1buckianNo ratings yet
- Requires Ongoing Support From Your Service: A Heart AttackDocument2 pagesRequires Ongoing Support From Your Service: A Heart AttackBîrlădeanu VlăduţNo ratings yet
- What Is A Physiatrist PowerpointDocument17 pagesWhat Is A Physiatrist PowerpointsirniravNo ratings yet
- Post Insertion Complaints in Complete Dentures - A Never Ending SagaDocument8 pagesPost Insertion Complaints in Complete Dentures - A Never Ending SagaKrupali JainNo ratings yet
- Spiggle & Theis BrochureDocument8 pagesSpiggle & Theis BrochureHaag-Streit UK (HS-UK)No ratings yet
- An Essay On The End-Of-Life Care in ChildrenDocument4 pagesAn Essay On The End-Of-Life Care in ChildrenThinashe MaswahuNo ratings yet
- Form Standarisasi BMHP RSU Jampang Kulon 2020Document6 pagesForm Standarisasi BMHP RSU Jampang Kulon 2020Avrilia Fuji AstutiNo ratings yet
- Complication of Sinus DiseaseDocument27 pagesComplication of Sinus DiseaseukhuholicNo ratings yet
- Filosofi Kesehatan MasyarakatDocument4 pagesFilosofi Kesehatan MasyarakatJennilynn YusameNo ratings yet
- Asuhan Keperawatan Manajemen Laktasi Dengan PendeDocument118 pagesAsuhan Keperawatan Manajemen Laktasi Dengan PendeRositaNo ratings yet
- Prof Norhayati RMC KPJUCDocument18 pagesProf Norhayati RMC KPJUCtheskywlkrNo ratings yet
- Anesthesia ALL PDFDocument195 pagesAnesthesia ALL PDFYasir RasoolNo ratings yet
- DM 2021-0114 Guidelines On The MGMT and Admin of The Initial 600,000 Donated SARS-CoV-2 Vaccine (Vero Cell) Inactivated Coronavac (Sinovac) DosesDocument17 pagesDM 2021-0114 Guidelines On The MGMT and Admin of The Initial 600,000 Donated SARS-CoV-2 Vaccine (Vero Cell) Inactivated Coronavac (Sinovac) DosesRalph Julius MendozaNo ratings yet
- 09 ITLS PretestDocument6 pages09 ITLS PretestArlanosaurus100% (2)
- Journal of Medicinal Plants Research VolDocument19 pagesJournal of Medicinal Plants Research VolAtheena Jin Anjelle SeveroNo ratings yet
- Abilify Dosing GuideDocument2 pagesAbilify Dosing GuidemtassyNo ratings yet