You might also like
- 2021 11 Vasectomy User GuideDocument2 pages2021 11 Vasectomy User Guidefarjad Farjad hassanNo ratings yet
- Permanent Contraception: VasectomyDocument13 pagesPermanent Contraception: VasectomyGhie Lotero EvangelistaNo ratings yet
- IT 31 - DIDIT Male ContraceptionDocument58 pagesIT 31 - DIDIT Male ContraceptionRizkiDwiryantiNo ratings yet
- Permanent Family PlanningDocument24 pagesPermanent Family Planningsurajchavan231116No ratings yet
- Family Planning FinalDocument30 pagesFamily Planning FinalJHONESSA LAYOSNo ratings yet
- Vasectomy: What You Should KnowDocument2 pagesVasectomy: What You Should KnowDiego SergioNo ratings yet
- Vasectomy - Advantages and DisadvantagesDocument12 pagesVasectomy - Advantages and DisadvantagesAubrey BolodoNo ratings yet
- VasectomyDocument7 pagesVasectomyAwang Wibisono100% (1)
- VASECTOMYDocument10 pagesVASECTOMYxxegyzzNo ratings yet
- What You Need To Know: Sterilisation For Women and MenDocument13 pagesWhat You Need To Know: Sterilisation For Women and MendonnyawNo ratings yet
- Birth Control or Contraception: Note: Please Insert Pictures For All The MethodDocument10 pagesBirth Control or Contraception: Note: Please Insert Pictures For All The MethodAnonymous b0gP6mDaqNo ratings yet
- Repro SystemDocument57 pagesRepro SystemRosa DeveraNo ratings yet
- Permanent ContraceptionDocument8 pagesPermanent ContraceptionJean Mae DesquitadoNo ratings yet
- Definition VasectomyDocument3 pagesDefinition VasectomyAnggy Wardhini100% (1)
- Permanent Family Planning MethodsDocument5 pagesPermanent Family Planning MethodsRALPH ELVIN MACANLALAYNo ratings yet
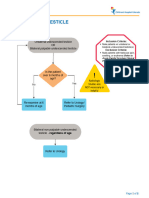
- Undescended Testicle PathwayDocument8 pagesUndescended Testicle PathwayJessa MaeNo ratings yet
- Family Planning - 5Document13 pagesFamily Planning - 5Khibul LimNo ratings yet
- Reproductive HealthDocument6 pagesReproductive HealthAdesh BhullarNo ratings yet
- Infertility, Contraception & AbortionDocument44 pagesInfertility, Contraception & AbortionaliciaisNo ratings yet
- Reproductive Health PowerNotes by KT SirDocument2 pagesReproductive Health PowerNotes by KT Sirjumihuss08No ratings yet
- Module 4 - Contraception and Family PlanningDocument18 pagesModule 4 - Contraception and Family PlanningKath NambuNo ratings yet
- ContraceptionDocument43 pagesContraceptionShivani TiwariNo ratings yet
- CircumcisionDocument18 pagesCircumcisionTriciaNo ratings yet
- VasectomyDocument4 pagesVasectomyBarry Quindoza RolluqueNo ratings yet
- Lec 4 Family Planning ProgramDocument23 pagesLec 4 Family Planning ProgramJohn Carlo ReyesNo ratings yet
- ContraceptionDocument34 pagesContraceptionMimo HemadNo ratings yet
- KB SterileDocument3 pagesKB Sterileauliarahma1254No ratings yet
- Methods of Family PlanningDocument46 pagesMethods of Family PlanningEyob MizanNo ratings yet
- Contraception - #2Document4 pagesContraception - #2Eingel Mer EvangelistaNo ratings yet
- ContraceptionDocument14 pagesContraceptionMunkhjin BayanmunkhNo ratings yet
- The Sexual Self Family PlanningDocument28 pagesThe Sexual Self Family PlanningShane UretaNo ratings yet
- Reviewer IiDocument34 pagesReviewer IigutierrezlycamNo ratings yet
- InfertilityDocument14 pagesInfertilityDrChauhanNo ratings yet
- Paediatric UrologyDocument194 pagesPaediatric UrologyTrishenth FonsekaNo ratings yet
- ContaceptionDocument66 pagesContaceptionSadaf AfzalNo ratings yet
- Family Planning and ContraceptivesDocument40 pagesFamily Planning and ContraceptivesJackie LegaspiNo ratings yet
- Sexual Reproduction-Methods of ContraceptionDocument14 pagesSexual Reproduction-Methods of Contraceptionshuanangs100% (1)
- Talis Sharma +2k Birth ControlDocument29 pagesTalis Sharma +2k Birth ControlTalis SharmaNo ratings yet
- Cervical Cerclage: About The Cervix in PregnancyDocument2 pagesCervical Cerclage: About The Cervix in Pregnancyamarendra Wardhana100% (1)
- Endometrial BiopsyDocument13 pagesEndometrial BiopsyChanta MaharjanNo ratings yet
- Contraceptive Methods HandoutsDocument14 pagesContraceptive Methods Handoutsapi-253521358No ratings yet
- Vaginal Hysterectomy and Vaginal Repair: Women's ServiceDocument16 pagesVaginal Hysterectomy and Vaginal Repair: Women's Serviceintan yulia safarinaNo ratings yet
- GRUP 4 AB FixDocument27 pagesGRUP 4 AB FixRosalita AtmaNo ratings yet
- Female SterilizationDocument2 pagesFemale SterilizationkgenilleNo ratings yet
- Presentation1 Cervical BiopsyDocument14 pagesPresentation1 Cervical BiopsyChanta MaharjanNo ratings yet
- Male InfertilityDocument19 pagesMale InfertilityUmer FarooqNo ratings yet
- VasectomyDocument5 pagesVasectomyNader SmadiNo ratings yet
- Solution Manual For Understanding Human Sexuality 14th Edition Janet Hydejohn DelamaterDocument37 pagesSolution Manual For Understanding Human Sexuality 14th Edition Janet Hydejohn DelamaterMarieHughesebgjp100% (80)
- ContraceptionDocument23 pagesContraceptionThilina KariyawasamNo ratings yet
- Womens Hormone BrochureDocument2 pagesWomens Hormone Brochurejuan antonio cruz velardeNo ratings yet
- Intimacy and Sexuality After Treatment For Gynecologic CancerDocument37 pagesIntimacy and Sexuality After Treatment For Gynecologic CancerCarleone PrimaNo ratings yet
- Bleeding During PregnancyDocument4 pagesBleeding During PregnancyCarl Andre ReyesNo ratings yet
- Undescended Testis, (Cryptorchidism) A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandUndescended Testis, (Cryptorchidism) A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (2)
- PhimosisDocument36 pagesPhimosisNamrata Karki100% (2)
- C2 Family PlanningDocument35 pagesC2 Family PlanningJency NithishajiNo ratings yet
- FAMILY PLanning FinalDocument23 pagesFAMILY PLanning FinalLebo Ramokolo100% (1)
- PD 5679 MisoprostolDocument2 pagesPD 5679 MisoprostolYuki-Pauline NagatoNo ratings yet
- Information For You: Pelvic Organ ProlapseDocument8 pagesInformation For You: Pelvic Organ Prolapsesandeepv08No ratings yet
- Diseases of BreastDocument33 pagesDiseases of BreastEggyDsNo ratings yet
- Hiperurisemia Dan Defisiensi Vit MineralDocument28 pagesHiperurisemia Dan Defisiensi Vit MineralEggyDsNo ratings yet
- Hiperurisemia Dan Defisiensi Vit MineralDocument28 pagesHiperurisemia Dan Defisiensi Vit MineralEggyDsNo ratings yet
- Hiperurisemia Dan Defisiensi Vit MineralDocument28 pagesHiperurisemia Dan Defisiensi Vit MineralEggyDsNo ratings yet
- Diseases of BreastDocument33 pagesDiseases of BreastEggyDsNo ratings yet
- Hipertensi KehamilanDocument37 pagesHipertensi KehamilanEggyDsNo ratings yet
- Patofisiologi MalariaDocument8 pagesPatofisiologi MalariaEggyDsNo ratings yet
- Endometrial HyperplasiaDocument21 pagesEndometrial HyperplasiaEggyDs100% (2)
- Ctopic Regnancy: Ehamilan KtopikDocument37 pagesCtopic Regnancy: Ehamilan KtopikEggyDsNo ratings yet
- Abnormality in NeonatesDocument30 pagesAbnormality in NeonatesEggyDsNo ratings yet
- Instructions For Completing The 3-Day Voiding DiaryDocument4 pagesInstructions For Completing The 3-Day Voiding DiaryAgil SaputraNo ratings yet
- Extracorporeal Shock Wave Lithotripsy (ESWL) vs. Ureterorenoscopic (URS) Manipulation in Proximal Ureteric StoneDocument5 pagesExtracorporeal Shock Wave Lithotripsy (ESWL) vs. Ureterorenoscopic (URS) Manipulation in Proximal Ureteric Stonealifah hainunNo ratings yet
- What Is A Urinary Tract InfectionDocument3 pagesWhat Is A Urinary Tract InfectionVanessa MendezNo ratings yet
- Urinary Tract Infections Core Curriculum 2024Document11 pagesUrinary Tract Infections Core Curriculum 2024Amanda EscorciaNo ratings yet
- Síndrome Adrenogenital e Alterações Anatômicas PDFDocument10 pagesSíndrome Adrenogenital e Alterações Anatômicas PDFFred SilvaNo ratings yet
- Bladder Training-Continence (Bladder) Training GoalDocument8 pagesBladder Training-Continence (Bladder) Training GoalYsabelle GutierrezNo ratings yet
- List of BSNL Empanelled Hospitals in AhmedabadDocument3 pagesList of BSNL Empanelled Hospitals in AhmedabadAnkit JaiswalNo ratings yet
- Nephrostomy ReportDocument4 pagesNephrostomy ReportPatrick Lloyd Merino Jackson100% (1)
- General Biology 2 Module 3.1 LASDocument3 pagesGeneral Biology 2 Module 3.1 LASX M O R T E M XNo ratings yet
- List of Empanelled HCOs - Delhi and NCR (30 Dec 2022)Document98 pagesList of Empanelled HCOs - Delhi and NCR (30 Dec 2022)Bhaskar MajumderNo ratings yet
- The Path Sperm-WPS OfficeDocument1 pageThe Path Sperm-WPS OfficeBryan Reufrir CortezanoNo ratings yet
- Various Styles of Sexual Intercourse (Ibg)Document16 pagesVarious Styles of Sexual Intercourse (Ibg)ravi4ramani62% (13)
- Diagnostic Criteria For UTI in Confused PatientDocument2 pagesDiagnostic Criteria For UTI in Confused PatientWallnut StreetNo ratings yet
- AnuriaDocument4 pagesAnuriachoobiNo ratings yet
- IPPS 2012 Program Book PDFDocument392 pagesIPPS 2012 Program Book PDFJanet L WarrenNo ratings yet
- A Comprehensie Study On Patient Satisfaction Towards: The Wockhardt HospitalDocument12 pagesA Comprehensie Study On Patient Satisfaction Towards: The Wockhardt HospitalPubg GamerNo ratings yet
- What Tests Are Done To Diagnose Kidney StonesDocument3 pagesWhat Tests Are Done To Diagnose Kidney StonesRatnaPrasadNalamNo ratings yet
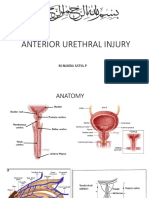
- Rupture Urethra Anterior DR Sule FixDocument36 pagesRupture Urethra Anterior DR Sule FixkadinfathiaNo ratings yet
- Acog Incontinencia Urinaria 2015Document16 pagesAcog Incontinencia Urinaria 2015amparoNo ratings yet
- Clinicopathological Profile and Outcome of Infection-Related Glomerulonephritis (Irgn) :a Single Center ExperienceDocument7 pagesClinicopathological Profile and Outcome of Infection-Related Glomerulonephritis (Irgn) :a Single Center ExperienceIJAR JOURNALNo ratings yet
- Seminar Epidemi HIV Indonesia - 10april2019 - C6Document59 pagesSeminar Epidemi HIV Indonesia - 10april2019 - C6Eny VeronikaNo ratings yet
- Homeopathic Remedies For Hydronephrosis - Homeo ExpertDocument7 pagesHomeopathic Remedies For Hydronephrosis - Homeo ExpertDr. Kazy Habibur RahmanNo ratings yet
- Bagian Kedua Tes Bahasa Inggris (NOMOR 121 S.D. 180) Structure and Written ExpressionDocument4 pagesBagian Kedua Tes Bahasa Inggris (NOMOR 121 S.D. 180) Structure and Written ExpressionamirahalimaNo ratings yet
- Intravenous UROGRAMDocument14 pagesIntravenous UROGRAMvijendrakumarsahuNo ratings yet
- New Text DocumentDocument2 pagesNew Text DocumenteqweNo ratings yet
- Tamsulosin RPS UK Apr 2016Document2 pagesTamsulosin RPS UK Apr 2016kolperrNo ratings yet
- What Is Glomerulonephritis?Document7 pagesWhat Is Glomerulonephritis?SSNo ratings yet
- Genital Surgical DiseasesDocument18 pagesGenital Surgical DiseasesanojNo ratings yet
- Urinary Tract InfectionsDocument35 pagesUrinary Tract InfectionsCharity Grace Magno100% (1)
- Deficient Knowledge Related To Urinary Tract Infection: "Di Ako Aware About Sa UTI"as Verbalized by The ClientDocument2 pagesDeficient Knowledge Related To Urinary Tract Infection: "Di Ako Aware About Sa UTI"as Verbalized by The ClientSeanmarie CabralesNo ratings yet