You might also like
- Internal Medicine Case Discussion on an Elderly Diabetic Patient with CoughDocument33 pagesInternal Medicine Case Discussion on an Elderly Diabetic Patient with CoughRobby GumawanNo ratings yet
- CBD Advisor Helps Elderly Patient With OrthopneaDocument38 pagesCBD Advisor Helps Elderly Patient With OrthopneaUmi RianaNo ratings yet
- Case of Hypertension, Diabetes and HeadacheDocument160 pagesCase of Hypertension, Diabetes and HeadacheJihan NabilaNo ratings yet
- CBD - Alifa Puspita P - 30101507367Document103 pagesCBD - Alifa Puspita P - 30101507367Jihan NabilaNo ratings yet
- History of IllnessDocument17 pagesHistory of IllnessChoirul UmamNo ratings yet
- CBD CHF Aziz 1.3 (Autosaved)Document75 pagesCBD CHF Aziz 1.3 (Autosaved)puspita widyaNo ratings yet
- CBD Fita DR Ana 123Document67 pagesCBD Fita DR Ana 123Fita Diyan ErikaNo ratings yet
- CBD Sirosis, Hematemesis MelenaDocument29 pagesCBD Sirosis, Hematemesis Melenadyah farahNo ratings yet
- Case Based Discussion: Supervisor: Dr. Nur Ana C, Sp. PD, KEMD, FINASIMDocument25 pagesCase Based Discussion: Supervisor: Dr. Nur Ana C, Sp. PD, KEMD, FINASIMFita Diyan ErikaNo ratings yet
- De Anisya Tri Ab - CBD - 30101507419 - FixDocument198 pagesDe Anisya Tri Ab - CBD - 30101507419 - FixFarah UlyaNo ratings yet
- Type 2 Diabetes, Neuropathy Case Discussion: Mr. TY (41Document47 pagesType 2 Diabetes, Neuropathy Case Discussion: Mr. TY (41Khenza Nur HasanahNo ratings yet
- CBD - Dr. H. M. Saugi Abduh, SP - PD, KKV, Finasim - Laode Muhammad Sukarno K - CHFDocument38 pagesCBD - Dr. H. M. Saugi Abduh, SP - PD, KKV, Finasim - Laode Muhammad Sukarno K - CHFkarnoNo ratings yet
- Case Based Discussion on Persistent Cough and HyperglycemiaDocument19 pagesCase Based Discussion on Persistent Cough and HyperglycemiaFita Diyan ErikaNo ratings yet
- CBD - DR Anna SP - PD - Robby Gunawan - P21.1Document14 pagesCBD - DR Anna SP - PD - Robby Gunawan - P21.1Robby GumawanNo ratings yet
- CBD Gastritis DR SaugiDocument36 pagesCBD Gastritis DR SaugiAlmira PratiwiNo ratings yet
- Case Based DiscussionDocument62 pagesCase Based DiscussionNeni SetyowatiNo ratings yet
- CBD DR Anna - Aulia Ayu SabillaDocument48 pagesCBD DR Anna - Aulia Ayu SabillaSandra MignonNo ratings yet
- CBD Nandaaji DR AnnaDocument10 pagesCBD Nandaaji DR AnnanandaajiNo ratings yet
- CBD Case Discussion on Abdominal Pain and IcterusDocument41 pagesCBD Case Discussion on Abdominal Pain and IcterusAnonymous 6MjSEwhOgcNo ratings yet
- Case Based Discussion: Advisor: Dr. H. Saugi Abduh, SP - PD, KKV, FINASIM Arranged By: Anisa Fauziah 30101306874Document45 pagesCase Based Discussion: Advisor: Dr. H. Saugi Abduh, SP - PD, KKV, FINASIM Arranged By: Anisa Fauziah 30101306874Almira PratiwiNo ratings yet
- CBD Sindroma Metabolik NinaDocument24 pagesCBD Sindroma Metabolik NinaNhinna Pinky'na BeibByNo ratings yet
- DR Saugi Nabila CBDDocument128 pagesDR Saugi Nabila CBDAmade DeaNo ratings yet
- CBD DR Anna - Talita HelgaDocument29 pagesCBD DR Anna - Talita Helgafais123No ratings yet
- MAN WITH ABDOMINAL PAIN AND LIVER MASSDocument77 pagesMAN WITH ABDOMINAL PAIN AND LIVER MASSMustika RanyNo ratings yet
- Case Based Discussion: Department of Internal Medicine Sultan Agung Islamic UniversityDocument40 pagesCase Based Discussion: Department of Internal Medicine Sultan Agung Islamic UniversitymaudiaNo ratings yet
- CBD DR Saugi - Monika SM-30101507496Document62 pagesCBD DR Saugi - Monika SM-30101507496Novi Dian LestariNo ratings yet
- Case Based Discussion: Pre-KDocument20 pagesCase Based Discussion: Pre-KAbd JalilNo ratings yet
- CBD Dr. Saugi - Robby GunawanDocument159 pagesCBD Dr. Saugi - Robby GunawanRobby GumawanNo ratings yet
- Case Based Discussion: Department of Internal Medicine Sultan Agung Islamic UniversityDocument209 pagesCase Based Discussion: Department of Internal Medicine Sultan Agung Islamic UniversityRiza Fadhila MuhammadNo ratings yet
- CBD DR Abah (Autosaved)Document73 pagesCBD DR Abah (Autosaved)Sindyputri HeldaNo ratings yet
- CBD DR SaugiDocument56 pagesCBD DR SaugiMohamad Reza HendratmokoNo ratings yet
- CBD Case Study on 67-Year-Old Male Farmer with DyspneaDocument68 pagesCBD Case Study on 67-Year-Old Male Farmer with DyspneaAditya Reza PrianugrahaNo ratings yet
- Case Based Discussion: Sindy Helda PutriDocument30 pagesCase Based Discussion: Sindy Helda PutriSindyputri HeldaNo ratings yet
- Case Base Discussion: Advisor: Dr. Nur Anna C Sa'dyah, Sp. PD, K-EMD, FINASIMDocument106 pagesCase Base Discussion: Advisor: Dr. Nur Anna C Sa'dyah, Sp. PD, K-EMD, FINASIMRiza Fadhila MuhammadNo ratings yet
- CBD HepatomaDocument201 pagesCBD HepatomafaridNo ratings yet
- Case Based Discussion: Ghulam Gilmani 012085663Document36 pagesCase Based Discussion: Ghulam Gilmani 012085663Ghulam GilmaniNo ratings yet
- Multiple Trauma Laporan KasusDocument13 pagesMultiple Trauma Laporan KasusAnantaahNo ratings yet
- CBD DR Anna SP - PD - Neni Setyowati (30101700126)Document12 pagesCBD DR Anna SP - PD - Neni Setyowati (30101700126)Neni SetyowatiNo ratings yet
- Case Based Discussion on Type 2 Diabetes MellitusDocument10 pagesCase Based Discussion on Type 2 Diabetes MellitusAulia Putri ANo ratings yet
- CBD Case Internal Medicine Heart DiseaseDocument30 pagesCBD Case Internal Medicine Heart DiseaseIlhamNo ratings yet
- 26-01-2022 Rabu - BPHDocument47 pages26-01-2022 Rabu - BPHRizal LuthfiNo ratings yet
- Sinus rhythmRateDocument84 pagesSinus rhythmRateIastNo ratings yet
- CBD CASE DISCUSSION ON HEPATIC ENCEPHALOPATHYDocument36 pagesCBD CASE DISCUSSION ON HEPATIC ENCEPHALOPATHYFatiya HidayatiNo ratings yet
- (Non Trauma) 02-07-2023 - Mrs. Etik - 58th - Colic UreterDocument12 pages(Non Trauma) 02-07-2023 - Mrs. Etik - 58th - Colic UreterRasyidu MashuriNo ratings yet
- CBD - Dr. Lusito, SP - PD - Nabilla Turista Lastanta - HEPATITIS B Obs. FebrisDocument13 pagesCBD - Dr. Lusito, SP - PD - Nabilla Turista Lastanta - HEPATITIS B Obs. Febriscrizt tyanNo ratings yet
- Tutorial Klinik: Dyspneu dan BronkopneumoniaDocument33 pagesTutorial Klinik: Dyspneu dan BronkopneumoniafemmytaniaNo ratings yet
- Case Based Disscusion: Rifqi Ali Zaki (01.208.5765) Advisor Dr. Erwin Budi Cahyono, Sp. PDDocument17 pagesCase Based Disscusion: Rifqi Ali Zaki (01.208.5765) Advisor Dr. Erwin Budi Cahyono, Sp. PDana0% (1)
- CBD - Kiki Bangun Wijaya - PPOKDocument13 pagesCBD - Kiki Bangun Wijaya - PPOKkiki WijayaNo ratings yet
- Case Based Discussion: Advisor: Dr. H. M. Saugi Abduh, SP - PD, KKV, FINASIMDocument33 pagesCase Based Discussion: Advisor: Dr. H. M. Saugi Abduh, SP - PD, KKV, FINASIMIlhamNo ratings yet
- (Case Based Discussion) A-55 Years Old Woman With Chest PainDocument56 pages(Case Based Discussion) A-55 Years Old Woman With Chest PainEnErin AnindithaNo ratings yet
- CBD Case DiscussionDocument35 pagesCBD Case DiscussionAramanda DianNo ratings yet
- GENERAL ANESTHESIA CASE REPORTDocument30 pagesGENERAL ANESTHESIA CASE REPORTMimin KurniaNo ratings yet
- Laporan Kasus Ileus ObstruksiDocument31 pagesLaporan Kasus Ileus ObstruksiRakha FahrezaNo ratings yet
- Laporan Jaga 5 Des 2018 DR - FeryDocument80 pagesLaporan Jaga 5 Des 2018 DR - FerygugimonNo ratings yet
- CKDDocument54 pagesCKDAnonymous UHnQSkxLBDNo ratings yet
- Case Based Discussion (CBD) : AdvisorDocument92 pagesCase Based Discussion (CBD) : AdvisorRiska Diene PratiwiNo ratings yet
- Case Based Discussion: Oquin Jastis Br. Damanik 30101206700Document41 pagesCase Based Discussion: Oquin Jastis Br. Damanik 30101206700Anonymous rgHszo9No ratings yet
- REFKAS - Dr. LusitoDocument43 pagesREFKAS - Dr. LusitoRizal LuthfiNo ratings yet
- A Randomized Controlled Trial of Zinc SupplementatDocument7 pagesA Randomized Controlled Trial of Zinc SupplementatRiantikaNo ratings yet
- SGD 1 LBM 2 22 SeptDocument8 pagesSGD 1 LBM 2 22 SeptRiantikaNo ratings yet
- Assessment ElektrolitDocument4 pagesAssessment ElektrolitRiantikaNo ratings yet
- SGD 1 LBM 2 22 SeptDocument8 pagesSGD 1 LBM 2 22 SeptRiantikaNo ratings yet
- WHO HIV Clinical Staging GuidelinesDocument49 pagesWHO HIV Clinical Staging Guidelinesdonovandube8235No ratings yet
- Mata LBM 2Document4 pagesMata LBM 2RiantikaNo ratings yet
- Agency For Toxic Substances and Disease Registry Case Studies in Environmental Medicine Cholinesterase InhibitorsDocument153 pagesAgency For Toxic Substances and Disease Registry Case Studies in Environmental Medicine Cholinesterase InhibitorsRiantikaNo ratings yet
- Riantika LBM 5 THTDocument48 pagesRiantika LBM 5 THTRiantikaNo ratings yet
- Riantika LBM 1 THTDocument73 pagesRiantika LBM 1 THTRiantikaNo ratings yet
- ABC of Liver Pancreas and Gall BladderDocument65 pagesABC of Liver Pancreas and Gall BladderMayer Rosenberg100% (3)
- Riantika LBM 1 MataDocument61 pagesRiantika LBM 1 MataRiantikaNo ratings yet
- Riantika LBM 5 THTDocument48 pagesRiantika LBM 5 THTRiantikaNo ratings yet
- ABC of Liver Pancreas and Gall BladderDocument65 pagesABC of Liver Pancreas and Gall BladderMayer Rosenberg100% (3)
- Riantika LBM 2 MataDocument54 pagesRiantika LBM 2 MataRiantikaNo ratings yet
- Filtrair Filter Media VNF M1 Series ENDocument2 pagesFiltrair Filter Media VNF M1 Series ENThái Hòa GiangNo ratings yet
- HP DeskJet Report POM 20150413Document5 pagesHP DeskJet Report POM 20150413Carolina DelgadoNo ratings yet
- Hydro-, Balneo-, and Spa Treatment in Pain Management PDFDocument5 pagesHydro-, Balneo-, and Spa Treatment in Pain Management PDFfriend717100% (1)
- I PU Assignment 2023-24 For WorkshopDocument12 pagesI PU Assignment 2023-24 For Workshopfaruff111100% (1)
- Evaluation of Sensors: For Mine Fire Detection Using An Atmospheric Monitoring SystemDocument9 pagesEvaluation of Sensors: For Mine Fire Detection Using An Atmospheric Monitoring SystemMario GaitanNo ratings yet
- Different Project Topics of BSNLDocument3 pagesDifferent Project Topics of BSNLAbhijit Tripathy0% (1)
- Frequency-Domain Analysis of Discrete-Time Signals and SystemsDocument31 pagesFrequency-Domain Analysis of Discrete-Time Signals and SystemsSwatiSharmaNo ratings yet
- Air Pollution Sources & EffectsDocument2 pagesAir Pollution Sources & EffectsJoanne Ash MajdaNo ratings yet
- Rodriguez ViereaDocument51 pagesRodriguez ViereaAwawawawa UwuwuwuwuNo ratings yet
- The Process, Church of The Final Judgment - ScripturesDocument132 pagesThe Process, Church of The Final Judgment - Scripturescirclesphere100% (2)
- Ase Utra Military and Law Enforcement ProductsDocument12 pagesAse Utra Military and Law Enforcement ProductsjamesfletcherNo ratings yet
- Mischel2004 - Toward An Integrative Science of The PersonDocument24 pagesMischel2004 - Toward An Integrative Science of The PersonTibor GalacziNo ratings yet
- Wall Mountable Switches - Wall Mounting GuideDocument3 pagesWall Mountable Switches - Wall Mounting GuideMarcos FilipeNo ratings yet
- Ic F3022SDocument36 pagesIc F3022SEfren.galNo ratings yet
- Chapter 2 - Coordinate GeometryDocument73 pagesChapter 2 - Coordinate GeometryFILIP CEZARNo ratings yet
- Hazardous Waste Identification GuidanceDocument105 pagesHazardous Waste Identification GuidanceMiguel TorresNo ratings yet
- 4.5.1.1 Inside and Outside Control Instructions - IG PDFDocument4 pages4.5.1.1 Inside and Outside Control Instructions - IG PDFMaksim Korsakov100% (4)
- Chapter 17Document48 pagesChapter 17MahmoudKhedrNo ratings yet
- 456/1 Mathematics Paper 1 June /july 2012 HoursDocument4 pages456/1 Mathematics Paper 1 June /july 2012 HoursBaguma MichaelNo ratings yet
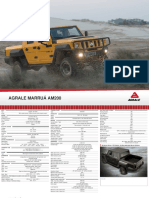
- Off Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Document2 pagesOff Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Victor SilvaNo ratings yet
- Modul 1 - Pengantar Remote SensingDocument60 pagesModul 1 - Pengantar Remote SensingNgurah Ade KalyanaNo ratings yet
- 12.3 Operation Qualification Protocol For Laminar Air Flow UnitDocument4 pages12.3 Operation Qualification Protocol For Laminar Air Flow UnituzairNo ratings yet
- WB City GateDocument7 pagesWB City GateDiegoNo ratings yet
- BhaishajyaDocument28 pagesBhaishajyadrsa2No ratings yet
- MAGA Training ReportDocument56 pagesMAGA Training ReportChaturanga WagaArachchige67% (3)
- Model146C DynamicGasCal 156file - 18125Document150 pagesModel146C DynamicGasCal 156file - 18125api-26966403100% (1)
- Intel Processors PDFDocument33 pagesIntel Processors PDFbiplab royNo ratings yet
- UL Anatomy 2022Document4 pagesUL Anatomy 2022jhom smithNo ratings yet
- Schutz - Subnotes PDFDocument47 pagesSchutz - Subnotes PDFJarryd RastiNo ratings yet
- Man and Mystery Vol 13 - Monsters and Cryptids (Rev06)Document139 pagesMan and Mystery Vol 13 - Monsters and Cryptids (Rev06)Pablo Jr AgsaludNo ratings yet