You might also like
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- Vincent B. VillaruzDocument160 pagesVincent B. VillaruzvincevilNo ratings yet
- Tips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointFrom EverandTips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointNo ratings yet
- Musculoskeletal SystemDocument124 pagesMusculoskeletal Systemnursereview93% (15)
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Traction Application Nursing ManagementDocument17 pagesTraction Application Nursing ManagementLatrell GelacioNo ratings yet
- Power Flex Stretching - Super Flexibility and Strength for peak performanceFrom EverandPower Flex Stretching - Super Flexibility and Strength for peak performanceRating: 3 out of 5 stars3/5 (3)
- Musculoskeletal-System NLE ReviewDocument124 pagesMusculoskeletal-System NLE ReviewRitamaria0% (1)
- Regaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryFrom EverandRegaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryNo ratings yet
- The Musculoskeletal HandoutsDocument3 pagesThe Musculoskeletal Handouts_Advernice_No ratings yet
- MusculoskeletalDocument40 pagesMusculoskeletalseigelystic100% (14)
- Traction & Application of p0pDocument19 pagesTraction & Application of p0pSham NazrinNo ratings yet
- Musculoskeletal Disorders: Prepared By: John Gil B. Ricafort, RNDocument55 pagesMusculoskeletal Disorders: Prepared By: John Gil B. Ricafort, RNPaola AgustinNo ratings yet
- Musculoskeletal SystemDocument10 pagesMusculoskeletal SystemPinky CuaresmaNo ratings yet
- Ortho AssignmentDocument18 pagesOrtho AssignmentSean Derick Cariño MercadoNo ratings yet
- TRACTIONSDocument29 pagesTRACTIONSRoeder CuerdaNo ratings yet
- Management of Musculoskeletal DisordersDocument69 pagesManagement of Musculoskeletal DisordersJSeasharkNo ratings yet
- Adm Traction PDFDocument10 pagesAdm Traction PDFbitha p bNo ratings yet
- Managing A Patient in CastDocument9 pagesManaging A Patient in CastIan RamaNo ratings yet
- Level of Student - B.SC (N) Ii Yrs Traction: Presented byDocument7 pagesLevel of Student - B.SC (N) Ii Yrs Traction: Presented bydhanasundariNo ratings yet
- Indirani College of Nursing: Level of Student - B.SC (N) Ii Yrs TractionDocument7 pagesIndirani College of Nursing: Level of Student - B.SC (N) Ii Yrs TractiondhanasundariNo ratings yet
- LilianDocument5 pagesLilianLilian Laureto SabinesNo ratings yet
- Musculoskeletal SystemDocument46 pagesMusculoskeletal Systemapi-3735995100% (2)
- TRACTION LavlyDocument9 pagesTRACTION Lavlylabsky_evol100% (1)
- Traction PPT FinalDocument26 pagesTraction PPT FinalMaryam saleemNo ratings yet
- Care of Patients With Traction NewDocument17 pagesCare of Patients With Traction Newjohnpantinople100% (17)
- Is The Use of A Pulling Force To Treat Muscle and Skeleton DisordersDocument42 pagesIs The Use of A Pulling Force To Treat Muscle and Skeleton DisordersShane Arianne Faye BaldoveNo ratings yet
- Musculoskeletal System Musculoskeletal System: A. SkeletonDocument23 pagesMusculoskeletal System Musculoskeletal System: A. SkeletonTina TalmadgeNo ratings yet
- Surgery - Care of Casts and TractionsDocument7 pagesSurgery - Care of Casts and TractionsMaria Eleni ÖNo ratings yet
- Activity22 (Traction)Document5 pagesActivity22 (Traction)Gabbii CincoNo ratings yet
- 3 Modalities (Traction, Fixator and Surgery)Document57 pages3 Modalities (Traction, Fixator and Surgery)Maria Lynne ParambitaNo ratings yet
- Applying and Managing Casts and TractionDocument13 pagesApplying and Managing Casts and TractionHampson MalekanoNo ratings yet
- NCP Self Care DeficitDocument15 pagesNCP Self Care DeficitSkye M. PetersNo ratings yet
- MS Musculoskeletal ReviewDocument12 pagesMS Musculoskeletal ReviewShayesra-Radina Laja SahibadNo ratings yet
- Skin TractionDocument5 pagesSkin TractionSuharyono100% (1)
- Mus Culo SkeletalDocument26 pagesMus Culo SkeletalCristy Ellain EsparteroNo ratings yet
- Amputation 4th YearDocument57 pagesAmputation 4th Yearshubham raulNo ratings yet
- Fractures, Dislocations, and Long-Duration Muscle Spasms, and To Prevent or Correct Deformities. TractionDocument2 pagesFractures, Dislocations, and Long-Duration Muscle Spasms, and To Prevent or Correct Deformities. TractionMarlon Rey AnacletoNo ratings yet
- Defining Traction and Fixation TermsDocument25 pagesDefining Traction and Fixation Termsmftaganas100% (1)
- FUNDA REVIEW 2 Body MechanicsDocument27 pagesFUNDA REVIEW 2 Body Mechanicslovie dooNo ratings yet
- Traction: Yasmin Samy Fouad Mohammed AttiaDocument20 pagesTraction: Yasmin Samy Fouad Mohammed AttiaAhmad YaseenNo ratings yet
- Nursing Traction TechniquesDocument10 pagesNursing Traction TechniquesSaniNo ratings yet
- Musculoskeletal - Student Review Questions Answers - DeWitDocument9 pagesMusculoskeletal - Student Review Questions Answers - DeWitkelsey jenningsNo ratings yet
- Fracture and CastDocument6 pagesFracture and Castmelissa guillermoNo ratings yet
- The Musculoskeletal System...Document24 pagesThe Musculoskeletal System...Charity Grace Magno67% (3)
- Body Mec and Bed MakingDocument95 pagesBody Mec and Bed Makingloise100% (1)
- Knee Arthroscopy Meniscectomy Recovery GuideDocument9 pagesKnee Arthroscopy Meniscectomy Recovery Guidebayan salahNo ratings yet
- Physiotherapy Goals and Techniques for Burn PatientsDocument15 pagesPhysiotherapy Goals and Techniques for Burn PatientsPraneetha NouduriNo ratings yet
- Cervical TractionDocument4 pagesCervical TractionGabbii CincoNo ratings yet
- wk2 FinTypes - of - Traction PDFDocument47 pageswk2 FinTypes - of - Traction PDFclaire yowsNo ratings yet
- Nursing RehabilitationDocument55 pagesNursing Rehabilitationnursereview100% (6)
- JP JP JP JPDocument7 pagesJP JP JP JPLean Ashly Tuddao MacarubboNo ratings yet
- Post-operative and Pre-Prosthetic Management for AmputeesDocument38 pagesPost-operative and Pre-Prosthetic Management for AmputeesTanzeelah RajawNo ratings yet
- Physiotherapy in AmputationsDocument6 pagesPhysiotherapy in Amputationskrissh20No ratings yet
- Modul PlusDocument64 pagesModul PlusMuhamad BenyaminNo ratings yet
- Traction NursingDocument75 pagesTraction NursingSujith KuttanNo ratings yet
- Inroduction To AmputationDocument67 pagesInroduction To AmputationAlfred JacksonNo ratings yet
- Balance Skeletal Traction1Document31 pagesBalance Skeletal Traction1Maria Victoria ColomaNo ratings yet
- Physiotherapy Rehabilitation Guidelines - Knee ArthrosDocument7 pagesPhysiotherapy Rehabilitation Guidelines - Knee ArthrosmatameaNo ratings yet
- NCP BkaDocument4 pagesNCP BkaKeeshia CesnerosNo ratings yet
- SamDocument1 pageSamIlhan RascalNo ratings yet
- Gastro Intestinal SytemDocument13 pagesGastro Intestinal SytemIlhan RascalNo ratings yet
- Drug Guide for NursesDocument2 pagesDrug Guide for NursesrihamNo ratings yet
- Preoperative NRSGDocument7 pagesPreoperative NRSGIlhan RascalNo ratings yet
- Community Health Nursing Practice Questions With RationalesDocument15 pagesCommunity Health Nursing Practice Questions With RationalesFelice Lamzon Labrador100% (2)
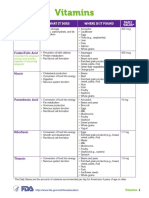
- Vitamins and Minerals GuideDocument5 pagesVitamins and Minerals GuideHrithik Sai TummalaNo ratings yet
- The Pediatric Mandible I. A Primer On Growth and DevelopmentDocument10 pagesThe Pediatric Mandible I. A Primer On Growth and DevelopmentJulián David Ríos ZuluagaNo ratings yet
- Devsecops Course Content: Module-1 Devops BasicsDocument3 pagesDevsecops Course Content: Module-1 Devops Basicshelo nameNo ratings yet
- Design and Development of A Three Phase Induction Motor Drive Using Ni-MyrioDocument5 pagesDesign and Development of A Three Phase Induction Motor Drive Using Ni-MyriovinaykumaarNo ratings yet
- Nurs478 Healthcaredelivery Audrey GohDocument12 pagesNurs478 Healthcaredelivery Audrey Gohapi-316372858No ratings yet
- ProVent - MANN + HUMMEL ProVent - Oil Separator For Open and Closed Crankcase Ventilation SystemsDocument29 pagesProVent - MANN + HUMMEL ProVent - Oil Separator For Open and Closed Crankcase Ventilation SystemsJosephNo ratings yet
- Refrac 2Document20 pagesRefrac 2PawanNo ratings yet
- Microwave TubesDocument36 pagesMicrowave TubesHINDUSTAN KNOW 1No ratings yet
- Points - Discover More RewardsDocument1 pagePoints - Discover More RewardsMustapha El HajjNo ratings yet
- Try inDocument80 pagesTry inLedia EssamNo ratings yet
- Aminacid MetabolismDocument84 pagesAminacid MetabolismAaronJose100% (1)
- SOP - APS - PUR - 02A - Flow Chart For PurchaseDocument2 pagesSOP - APS - PUR - 02A - Flow Chart For Purchaseprakash patelNo ratings yet
- Wind Energy 6Document12 pagesWind Energy 6Shanthi RameshNo ratings yet
- RMO Orientation AIRMEDDocument130 pagesRMO Orientation AIRMEDqueenartemisNo ratings yet
- Global Leader: in Glass IonomerDocument2 pagesGlobal Leader: in Glass IonomerAnggini ZakiyahNo ratings yet
- SpamDocument2 pagesSpamAshutosh SinghNo ratings yet
- 2017 Aso Security TrainingDocument60 pages2017 Aso Security TrainingTanzila SiddiquiNo ratings yet
- Artificial Intelligence in Rheumatology: Applications and ChallengesDocument39 pagesArtificial Intelligence in Rheumatology: Applications and ChallengesMaryame BoutkhilNo ratings yet
- People Magazine Ronnie Van Zant 4Document1 pagePeople Magazine Ronnie Van Zant 4Randy CarterNo ratings yet
- Pds - Sunshades Instrument CoverDocument2 pagesPds - Sunshades Instrument CoverAntonio LantiguaNo ratings yet
- A300-600 Ammfx1 29 24 00 03 0Document5 pagesA300-600 Ammfx1 29 24 00 03 0Fahimeh HayatinasabNo ratings yet
- Biology 1Document4 pagesBiology 1yvonne villanuevaNo ratings yet
- End Time ProphecyDocument16 pagesEnd Time ProphecyMarven JabianNo ratings yet
- Sika Poxitar FDocument3 pagesSika Poxitar FBudhi KurniawanNo ratings yet
- English 1000 Most Repeated MCQs by Learning With Rizwan - 083731Document145 pagesEnglish 1000 Most Repeated MCQs by Learning With Rizwan - 083731Athleteboy7No ratings yet
- Medical Certificate: (Coaches, Assistant Coaches, Chaperone)Document1 pageMedical Certificate: (Coaches, Assistant Coaches, Chaperone)Keith Marinas Serquina100% (1)
- Specification for Child MUAC Tape Quality ChecksDocument4 pagesSpecification for Child MUAC Tape Quality ChecksM HussainNo ratings yet
- Flatworms Round Worms and Anne Lids LabDocument6 pagesFlatworms Round Worms and Anne Lids LabBellaNo ratings yet
- FT-IR Analysis of Hock ProcessDocument4 pagesFT-IR Analysis of Hock ProcessmohsengolestanzadehNo ratings yet
- 01 Itp-380kv Gis - PlanDocument9 pages01 Itp-380kv Gis - PlanYahya SamaraNo ratings yet
- Why encouraging entrepreneurship to boost economies is flawedDocument9 pagesWhy encouraging entrepreneurship to boost economies is flawedLaureanoNo ratings yet