You might also like
- 2017 STEMI Ehx393 - Web Addenda - For WEBDocument8 pages2017 STEMI Ehx393 - Web Addenda - For WEBRESCATEURNo ratings yet
- Reviewon CeftriaxoneDocument15 pagesReviewon CeftriaxoneJohny SevenfoldismNo ratings yet
- Reviewon CeftriaxoneDocument15 pagesReviewon CeftriaxoneJohny SevenfoldismNo ratings yet
- ZTRK 2013 OdettaDocument5 pagesZTRK 2013 OdettaJohny SevenfoldismNo ratings yet
- Biodiversity of Mollusks at Ela-Ela Beach SekotongDocument6 pagesBiodiversity of Mollusks at Ela-Ela Beach SekotongJohny SevenfoldismNo ratings yet
- MR 20-06-2019Document21 pagesMR 20-06-2019Johny SevenfoldismNo ratings yet
- MR 28-06-2019Document24 pagesMR 28-06-2019Johny SevenfoldismNo ratings yet
- Diosgenin: Other Names: (20R, 25R) - Spirost-5-En-3 Beta - OlDocument2 pagesDiosgenin: Other Names: (20R, 25R) - Spirost-5-En-3 Beta - OlJohny SevenfoldismNo ratings yet
- MR 28-06-2019Document24 pagesMR 28-06-2019Johny SevenfoldismNo ratings yet
- Bawang Putih 3Document8 pagesBawang Putih 3Johny SevenfoldismNo ratings yet
- Estimation of Time Since Death by Using Algorithm in Early Postmortem PeriodDocument31 pagesEstimation of Time Since Death by Using Algorithm in Early Postmortem PeriodJohny SevenfoldismNo ratings yet
- LemursssssssDocument8 pagesLemursssssssJohny SevenfoldismNo ratings yet
- Morning Report Dengan DR Yasa TGL 4 Juanuari 2019Document33 pagesMorning Report Dengan DR Yasa TGL 4 Juanuari 2019Johny SevenfoldismNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Assessment Diagnosis Outcomes Intervention Evaluation: Mabini Colleges, Inc. College of Nursing and MidwiferyDocument3 pagesAssessment Diagnosis Outcomes Intervention Evaluation: Mabini Colleges, Inc. College of Nursing and MidwiferyKathrina Mendoza HembradorNo ratings yet
- (Result) UPSC CAPF Assistant Commandant (AC) 2012 Result Announced (And PET Tips) MrunalDocument13 pages(Result) UPSC CAPF Assistant Commandant (AC) 2012 Result Announced (And PET Tips) Mrunalguru1241987babuNo ratings yet
- Approaches To Quality Management andDocument19 pagesApproaches To Quality Management andPhillip David Ormeño Vasquez100% (1)
- Iap Guidelines On Rickettsial Diseases in ChildrenDocument7 pagesIap Guidelines On Rickettsial Diseases in Childrenitaa19No ratings yet
- Ion Breeding Policy - 2006 & 2010Document42 pagesIon Breeding Policy - 2006 & 2010Ulhas GaikwadNo ratings yet
- Local Anaesthetics Mcqs From LouisDocument6 pagesLocal Anaesthetics Mcqs From LouisAmreen Khan100% (1)
- Surat Permintaan Obat Dinkes BaruDocument21 pagesSurat Permintaan Obat Dinkes BaruHafizh JhunkoNo ratings yet
- Definitions of Human SecurityDocument10 pagesDefinitions of Human SecurityClandestain Zee100% (2)
- Grade 9 Solid Waste Management Teachers - GuideDocument32 pagesGrade 9 Solid Waste Management Teachers - GuideNicole Angela NavarroNo ratings yet
- Zinc in Wound Healing Theoretical, ExperimentalDocument15 pagesZinc in Wound Healing Theoretical, ExperimentalRifky Budi TriyatnoNo ratings yet
- Vancomycin DRUGSTUDYDocument3 pagesVancomycin DRUGSTUDYEmagra AzilNo ratings yet
- Art Comparison Essay ExampleDocument5 pagesArt Comparison Essay Exampleflrzcpaeg100% (2)
- Dheeraj DumirDocument11 pagesDheeraj DumirAnonymous CR8v7xb0No ratings yet
- List of CosmeticsDocument9 pagesList of Cosmeticsasit_m0% (1)
- Minimizing The Risk of Alzheimer S DiseaseDocument328 pagesMinimizing The Risk of Alzheimer S DiseaseLuis Raudales100% (1)
- The Emergence of India's Pharmaceutical IndustryDocument41 pagesThe Emergence of India's Pharmaceutical Industryvivekgupta2jNo ratings yet
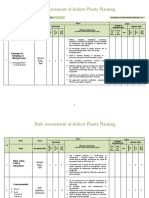
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Script NewscasterDocument1 pageScript NewscasterJuandito YudhatamaNo ratings yet
- MSDS Cim PremixDocument3 pagesMSDS Cim PremixKiệt Lê TuấnNo ratings yet
- Isu Dan Etika Pada Perawatan Paliatif PDFDocument17 pagesIsu Dan Etika Pada Perawatan Paliatif PDFNatasya ChieCaem FunforeverNo ratings yet
- Data Legacy InsuranceCos SourceRSDocument48 pagesData Legacy InsuranceCos SourceRSrishu1527No ratings yet
- KSCST PresentationDocument44 pagesKSCST PresentationAkshay SavvasheriNo ratings yet
- Learners With Difficulty CommunicatingDocument15 pagesLearners With Difficulty CommunicatingVhong ValleserNo ratings yet
- A Healthy Menopause: Diet, Nutrition and Lifestyle GuidanceDocument8 pagesA Healthy Menopause: Diet, Nutrition and Lifestyle GuidanceAnonymous bq4KY0mcWGNo ratings yet
- BD Product ListDocument48 pagesBD Product Listanish_10677953100% (1)
- Jhs Learner DataDocument3 pagesJhs Learner Dataapi-377500541No ratings yet
- Norma Ashrae 62 1989Document3 pagesNorma Ashrae 62 1989Mittzi CallejasNo ratings yet
- Gases Toxicos Irritantes PDFDocument6 pagesGases Toxicos Irritantes PDFLUIS ANDRES JUAREZ CALLENo ratings yet
- Nuevas Patologias Cie 10Document281 pagesNuevas Patologias Cie 10Ana guely santivañez mitmaNo ratings yet
- Assignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Document3 pagesAssignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Hafshah AgustinaNo ratings yet