You might also like
- Peduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Document11 pagesPeduc 01 PATH-Fit (Physical Activities Towards Health and Fitness) First Semester - School Year 2021 - 2022Grace BrigondoNo ratings yet
- MCQ NeuroDocument21 pagesMCQ NeuroMasayu Mutiara UtiNo ratings yet
- DR Bambang EnsefalitisDocument46 pagesDR Bambang EnsefalitisSemestaNo ratings yet
- Bacterial MeningitisDocument2 pagesBacterial Meningitisjennielunay00No ratings yet
- PyomeningitisDocument54 pagesPyomeningitisRiya BagdiNo ratings yet
- Meningitis and Fractures Concept MapDocument4 pagesMeningitis and Fractures Concept MapNamayanja SumayiyahNo ratings yet
- Dr. Dede Gunawan - CURRENT MANAGEMENT OF VIRAL ENCEPHALITIS (Rev)Document28 pagesDr. Dede Gunawan - CURRENT MANAGEMENT OF VIRAL ENCEPHALITIS (Rev)Adnin NugrohoNo ratings yet
- Kuliah Infeksi SSP 2021Document85 pagesKuliah Infeksi SSP 2021clarissaNo ratings yet
- MK Pen Slide EnsefalitisDocument19 pagesMK Pen Slide EnsefalitisUchy JurasuyunuNo ratings yet
- CNS Infection, ReviewsDocument17 pagesCNS Infection, ReviewsAbdulelah MurshidNo ratings yet
- Hiv Aids KemenkesDocument12 pagesHiv Aids KemenkesTasyaNo ratings yet
- LP EncephalitisDocument28 pagesLP EncephalitisAmar DoanxNo ratings yet
- Encephalitis ReportDocument4 pagesEncephalitis ReportMiss GNo ratings yet
- MeningitisDocument2 pagesMeningitisedrian02No ratings yet
- Definición, Etiología, Epidemiología, Patogenia Y FisiopatologíaDocument8 pagesDefinición, Etiología, Epidemiología, Patogenia Y FisiopatologíaGregorio BenitesNo ratings yet
- MeningitisDocument3 pagesMeningitisDiana Fadhilah SariNo ratings yet
- DPW (GBS VS TM)Document29 pagesDPW (GBS VS TM)Muhammad HerryNo ratings yet
- Infection 2Document35 pagesInfection 2Anuj PatelNo ratings yet
- AAAA2Document142 pagesAAAA2Sruthi SruthiNo ratings yet
- CNS Infections Aug 2022 Harsha - 2nd DraftDocument106 pagesCNS Infections Aug 2022 Harsha - 2nd Draftharsha sinhaNo ratings yet
- Meningitis and Encephalitis: PGI Roddame Angelo ErispeDocument100 pagesMeningitis and Encephalitis: PGI Roddame Angelo ErispeAngelo ErispeNo ratings yet
- rUVm2KdohoeaEVlJZJkS1601096552 PDFDocument32 pagesrUVm2KdohoeaEVlJZJkS1601096552 PDFAsfiksia NeonatorumNo ratings yet
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
- Appr FeverDocument2 pagesAppr FeverThitanun TungchutworakulNo ratings yet
- 3.3 NEUROSENSORY DISORDERS Mikrobiologi 2018-2019 RRDocument202 pages3.3 NEUROSENSORY DISORDERS Mikrobiologi 2018-2019 RRHirotaka KitabatakeNo ratings yet
- Spina Bifida 2: NeuroDocument16 pagesSpina Bifida 2: NeuroluckyariadneeNo ratings yet
- Central Nervous System Infection (Infeksi Susunan Saraf Pusat)Document92 pagesCentral Nervous System Infection (Infeksi Susunan Saraf Pusat)Farihatun NisaNo ratings yet
- Central Nervous System Pathology: Presented byDocument70 pagesCentral Nervous System Pathology: Presented byNicholasNo ratings yet
- Meningitis, Encephalitis and Brain Abscess: by D OgoinaDocument62 pagesMeningitis, Encephalitis and Brain Abscess: by D OgoinaPrincewill SeiyefaNo ratings yet
- Ataxia PresentationDocument11 pagesAtaxia PresentationS RiarNo ratings yet
- Bacterial MeningitisDocument2 pagesBacterial Meningitisjennielunay00No ratings yet
- MeningitisDocument17 pagesMeningitisKyla Marie TejadaNo ratings yet
- Exámenes Auxiliares: NeurologíaDocument12 pagesExámenes Auxiliares: NeurologíaHugo CardenasNo ratings yet
- Bacterial MeningitisDocument40 pagesBacterial MeningitisDinesh ReddyNo ratings yet
- Acute Meningitis: DR K. Saroj Novel Jr-1 General Medicine Moderator:Dr - Sushanth MD Assistant ProfessorDocument28 pagesAcute Meningitis: DR K. Saroj Novel Jr-1 General Medicine Moderator:Dr - Sushanth MD Assistant ProfessorSaikiran GundaboynaNo ratings yet
- Pediatric CNS InfectionsDocument105 pagesPediatric CNS InfectionsDan Matthew BuriasNo ratings yet
- Session 4 With AudioDocument28 pagesSession 4 With Audioshaanika1502No ratings yet
- LP After Correct.Document32 pagesLP After Correct.Academic Nurse. M.M AbbasNo ratings yet
- Pediatric Systemic Lupus ErythematosusDocument35 pagesPediatric Systemic Lupus ErythematosusJames Abram GuardiarioNo ratings yet
- REFRAT SARAF HNPDocument16 pagesREFRAT SARAF HNPKamalAbdurrosidRosidNo ratings yet
- Pathogenesis of MENINGITISDocument30 pagesPathogenesis of MENINGITISPrachi TeteNo ratings yet
- 10 - Disorders of Consciousness and Language I (Coma and Confusional States) LectureDocument119 pages10 - Disorders of Consciousness and Language I (Coma and Confusional States) LectureRanjit SharmaNo ratings yet
- Herpes Zoster: Nurul Iska Ulmarika Idrisc111 10 831 Ruth Faustine J. Rayo C 1 1 1 1 0 1 8 0Document26 pagesHerpes Zoster: Nurul Iska Ulmarika Idrisc111 10 831 Ruth Faustine J. Rayo C 1 1 1 1 0 1 8 0fatqur280% (1)
- (Neuro) 016 Cns-InfectionDocument18 pages(Neuro) 016 Cns-Infection3BBEGILJUDY ANNBNo ratings yet
- Encephalitis Nursing Case StudyDocument7 pagesEncephalitis Nursing Case StudyJitendraNo ratings yet
- High Fever Stiff Neck Severe HeadacheDocument3 pagesHigh Fever Stiff Neck Severe HeadacheDiana Jane LauretaNo ratings yet
- (123doc) - Thuc-Hanh-Dich-2-Thay-Nguyen-Viet-Ki-Unit-6-MedicineDocument11 pages(123doc) - Thuc-Hanh-Dich-2-Thay-Nguyen-Viet-Ki-Unit-6-MedicineLê Thị NhưÝNo ratings yet
- Bacterial MeningitisDocument37 pagesBacterial MeningitisMission JupiterNo ratings yet
- Gbs (Guillain Barre Syndrome)Document16 pagesGbs (Guillain Barre Syndrome)Mimba Wibiyana100% (1)
- Enchepalitis in Pediatric PopulationDocument14 pagesEnchepalitis in Pediatric PopulationAdityaWigunaNo ratings yet
- Neurological Infections: By, Mr. Anish Ghosh M.Sc. Nursing 2 YearDocument57 pagesNeurological Infections: By, Mr. Anish Ghosh M.Sc. Nursing 2 YearAnish GhoshNo ratings yet
- Encephalitis Brain Abscess: Reşat Özaras, MD, Prof. Infection DeptDocument45 pagesEncephalitis Brain Abscess: Reşat Özaras, MD, Prof. Infection DeptChristian KennethNo ratings yet
- Pathogenesis of The Central Nervous System InfectionDocument44 pagesPathogenesis of The Central Nervous System InfectionMira ApriliaNo ratings yet
- Laporan Pendahuluan Pada Pasien Space Occupying Lesion (Sol) SerebriDocument20 pagesLaporan Pendahuluan Pada Pasien Space Occupying Lesion (Sol) SerebriNovi WinriNo ratings yet
- What Is Meningitis?Document7 pagesWhat Is Meningitis?laujeroNo ratings yet
- Seizure Associated With Corona Virus Infection: Meiti Frida PERDOSSI Cabang PadangDocument23 pagesSeizure Associated With Corona Virus Infection: Meiti Frida PERDOSSI Cabang Padangzefri suhendarNo ratings yet
- Virus Zoster, Enterovirus,: Problem TreeDocument3 pagesVirus Zoster, Enterovirus,: Problem TreeIhtiramiNo ratings yet
- EncephalitisDocument17 pagesEncephalitisanshitaNo ratings yet
- Neuro Infectii Ghid ClinicDocument74 pagesNeuro Infectii Ghid ClinicEnzo de PalmaNo ratings yet
- Guarin - Inflammatory Disturbances NotesDocument6 pagesGuarin - Inflammatory Disturbances NotesMary Joy Anne LucasNo ratings yet
- Encephalitis, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandEncephalitis, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (16)
- Delay Umbilical 2Document6 pagesDelay Umbilical 2Sisrini Rahayu SammarianNo ratings yet
- First Problem: Group 14 27 September 2018Document52 pagesFirst Problem: Group 14 27 September 2018RioNo ratings yet
- 14 FirstproblemDocument52 pages14 FirstproblemSilvia CreSiaNo ratings yet
- Delay Umbilical 2Document6 pagesDelay Umbilical 2Sisrini Rahayu SammarianNo ratings yet
- Fifth Problem - LouisDocument99 pagesFifth Problem - LouisRioNo ratings yet
- Problem 06: Group 04 Monday, 28 October 2019Document53 pagesProblem 06: Group 04 Monday, 28 October 2019RioNo ratings yet
- Comparing The Diagnostic Accuracy of 3 Ultrasound Modalities For Diagnosing Obstetric Anal Sphincter InjuriesDocument9 pagesComparing The Diagnostic Accuracy of 3 Ultrasound Modalities For Diagnosing Obstetric Anal Sphincter InjuriesRioNo ratings yet
- Management of HypertensionDocument6 pagesManagement of HypertensionRioNo ratings yet
- Summary LouisDocument16 pagesSummary LouisRioNo ratings yet
- Antibiotik Dan AntifungalDocument1 pageAntibiotik Dan AntifungalRioNo ratings yet
- Department of Education: Granja Kalinawan National High SchoolDocument26 pagesDepartment of Education: Granja Kalinawan National High SchoolRoselyn Mae DulaNo ratings yet
- Sugar Free Shopping ListDocument4 pagesSugar Free Shopping Listhsquiers100% (3)
- Jakarta Declaration PPDocument17 pagesJakarta Declaration PPvashniNo ratings yet
- 48069B - Ferrofos 5260 (GB-ENG)Document6 pages48069B - Ferrofos 5260 (GB-ENG)danielNo ratings yet
- Internship PresentationDocument23 pagesInternship Presentationapi-556937362No ratings yet
- Ethiopian Chicken (Doro Wat Stew) Recipe - FoodDocument2 pagesEthiopian Chicken (Doro Wat Stew) Recipe - FoodPalomequeNo ratings yet
- List of CosmeticsDocument9 pagesList of Cosmeticsasit_m0% (1)
- Transdiagnostic TreatmentDocument9 pagesTransdiagnostic Treatmentvalentina chistrugaNo ratings yet
- Gases Toxicos Irritantes PDFDocument6 pagesGases Toxicos Irritantes PDFLUIS ANDRES JUAREZ CALLENo ratings yet
- Sensory Design of Easy-To-Chew Food For Elderly: - Ingredients and Manufacturing Conditions With Focus On Meat and CarrotDocument23 pagesSensory Design of Easy-To-Chew Food For Elderly: - Ingredients and Manufacturing Conditions With Focus On Meat and CarrotCaguioa Mark Anthony G.No ratings yet
- Chapter 01Document22 pagesChapter 01kita5437100% (1)
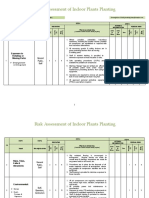
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Konsolidasi WelmiDocument72 pagesKonsolidasi WelmiWelmi Sulfatri IshakNo ratings yet
- Primary Eye Care-A Manual For Health WorkersDocument76 pagesPrimary Eye Care-A Manual For Health WorkersRHU LOOCNo ratings yet
- Anupama Ra NotesDocument23 pagesAnupama Ra NotesShahzeel Iftikhar100% (1)
- Study Guide For Pathophysiology The Biological Basis Disease in Adults and Ebook PDF VersionDocument58 pagesStudy Guide For Pathophysiology The Biological Basis Disease in Adults and Ebook PDF Versionalfred.jessie484100% (38)
- A Handbook of Dementia Care: Edited byDocument15 pagesA Handbook of Dementia Care: Edited byJovana Ognenovska Bakalovska100% (1)
- JUVENILE Justice ProjectDocument24 pagesJUVENILE Justice ProjectyashaNo ratings yet
- Hematology EMQDocument7 pagesHematology EMQfrabzi100% (1)
- Bahasa Inggris Swot Madam Gie Sweet Cheek BlushedDocument8 pagesBahasa Inggris Swot Madam Gie Sweet Cheek Blushedanon_681594518No ratings yet
- HSE National Cleaning Standards ManualDocument149 pagesHSE National Cleaning Standards ManualNemer MansourNo ratings yet
- Alice in Michigan: A Financial Hardship StudyDocument58 pagesAlice in Michigan: A Financial Hardship StudydaneNo ratings yet
- Impaired Posture and MovementDocument40 pagesImpaired Posture and MovementMohamed Magdy ElMeligieNo ratings yet
- Sip 2Document112 pagesSip 2harnishaNo ratings yet
- Unit 3Document15 pagesUnit 3Neenu RajputNo ratings yet
- Pengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseDocument9 pagesPengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseTjatur SurantullohNo ratings yet
- ARC 360 NGP InstructionManualDocument24 pagesARC 360 NGP InstructionManualLMTNo ratings yet
- Allan ALH105 Week 3Document5 pagesAllan ALH105 Week 3alvin mwizNo ratings yet
- Bajaj Allianz General Insurance Company LTD.: Declaration by The InsuredDocument1 pageBajaj Allianz General Insurance Company LTD.: Declaration by The InsuredArtiNo ratings yet